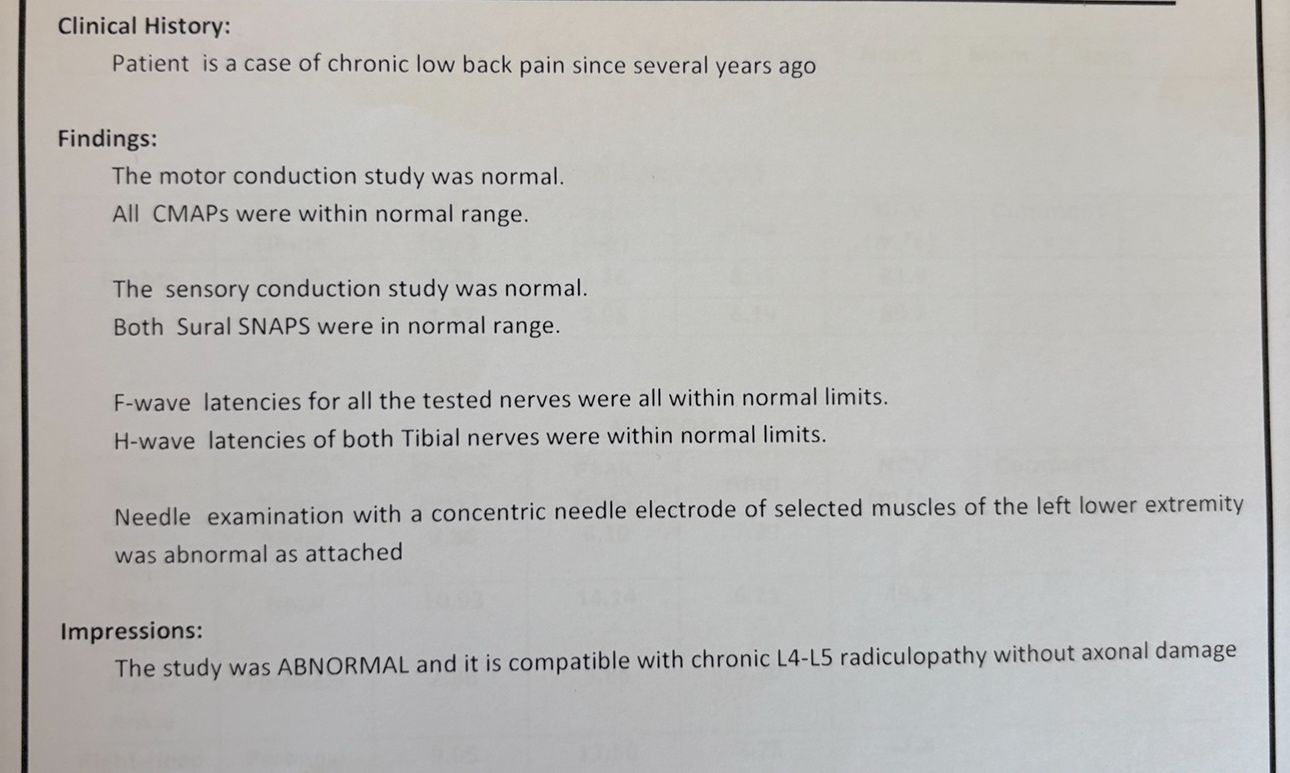
Articles, Lectures, my own patients presentations with their MRI before/after chiropractic treatment by DR. Cyrus
MRI of patients who have improved after chiropractic treatment by DR. Cyrus Salimian
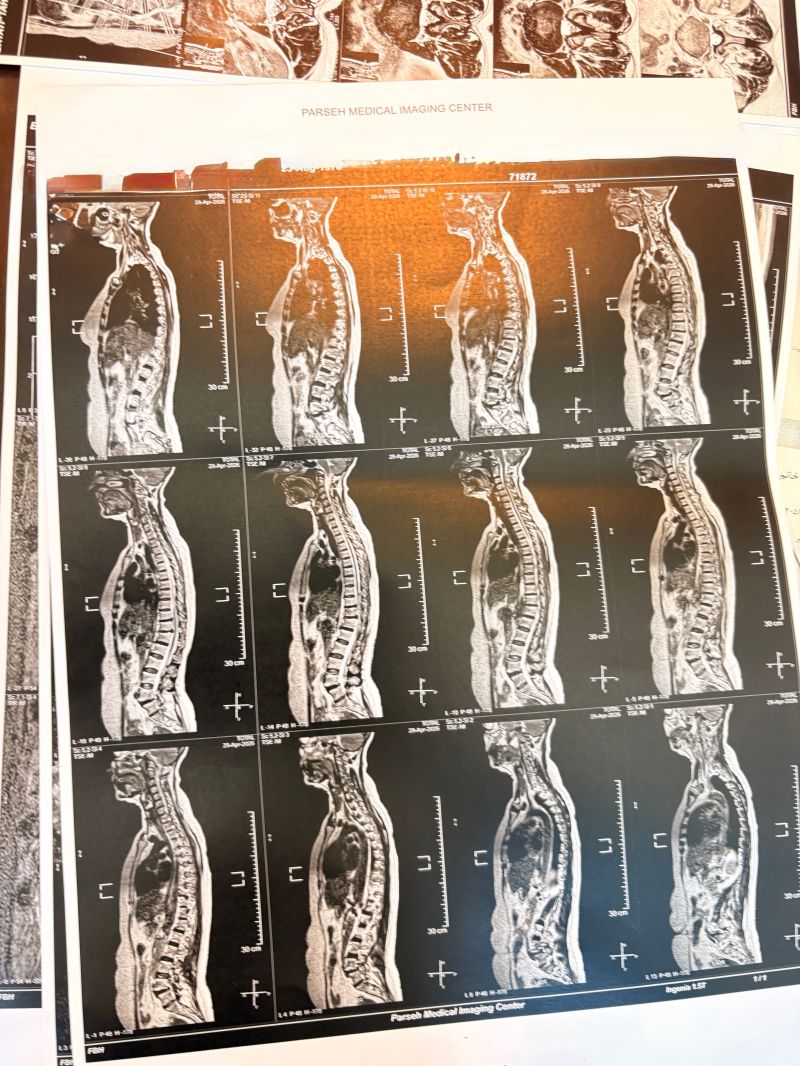
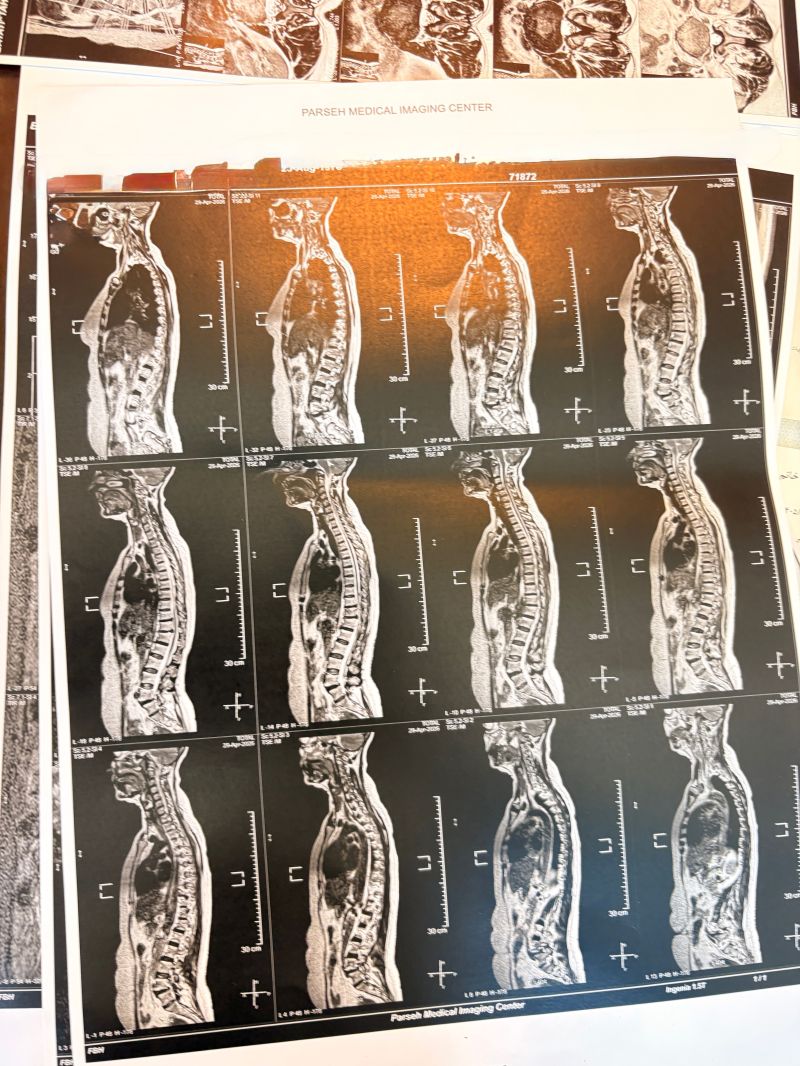
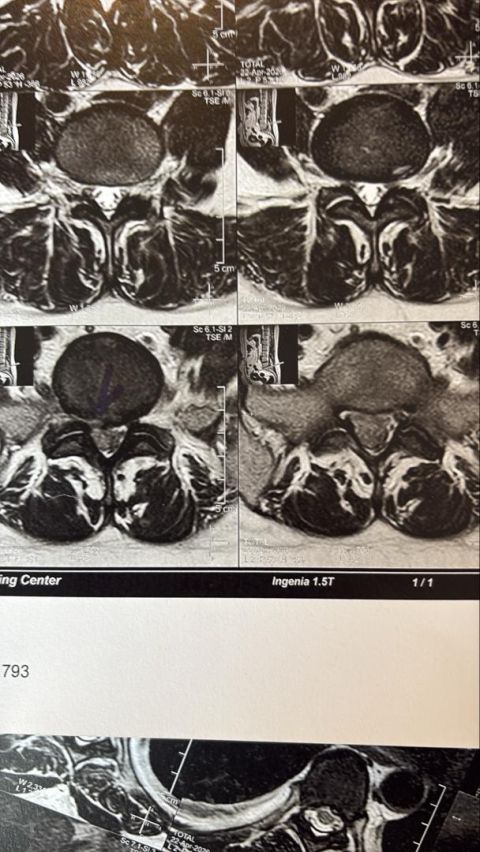
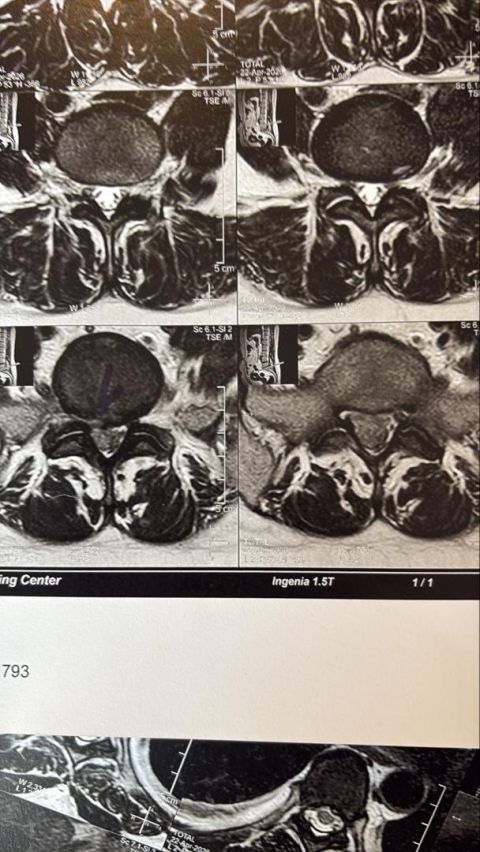
Case 1
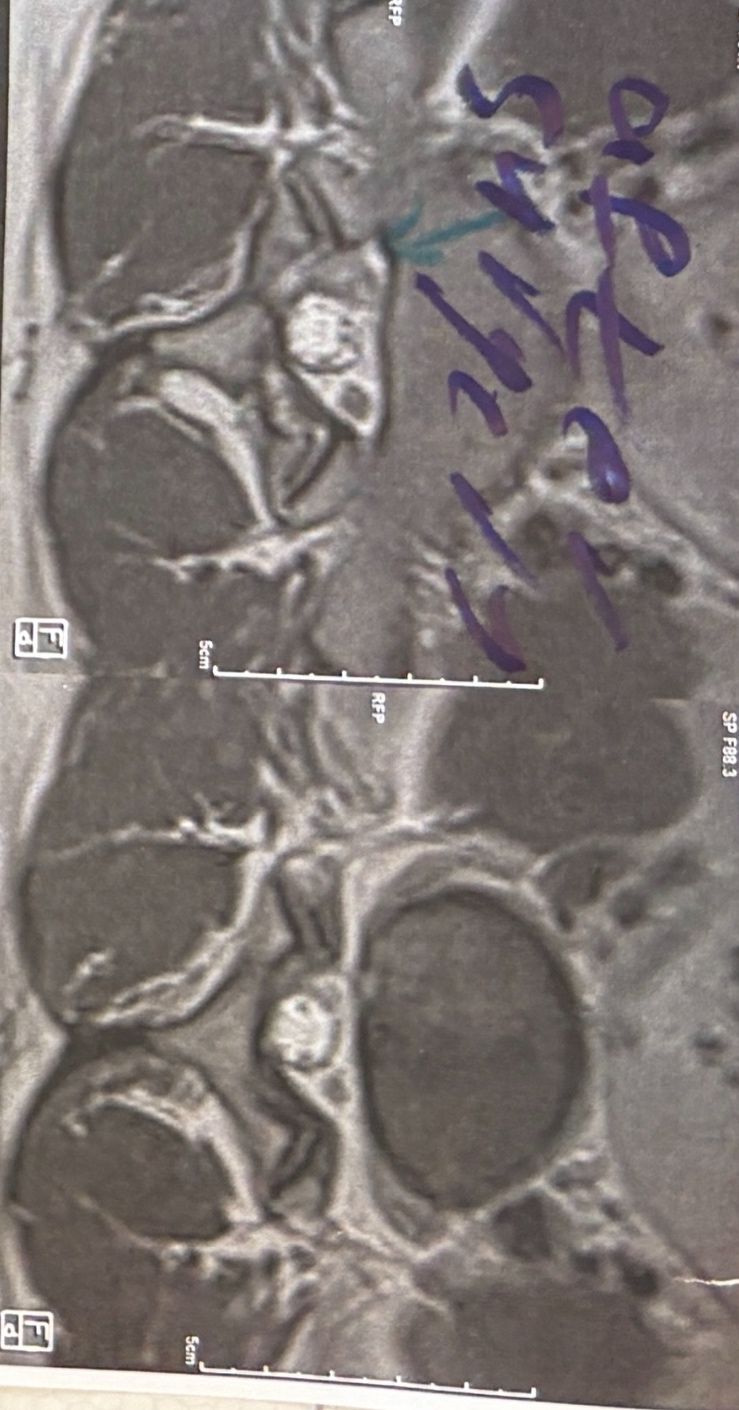
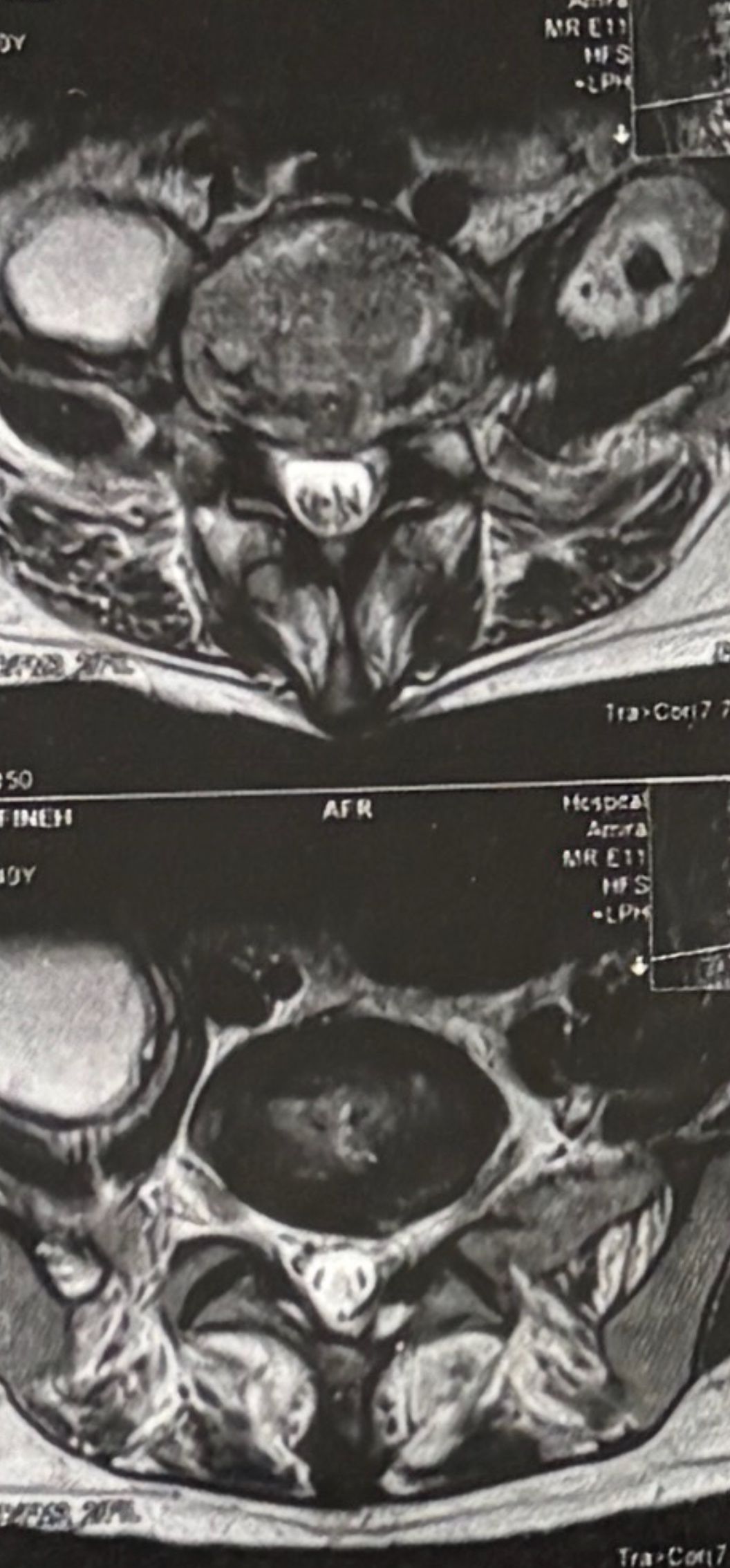
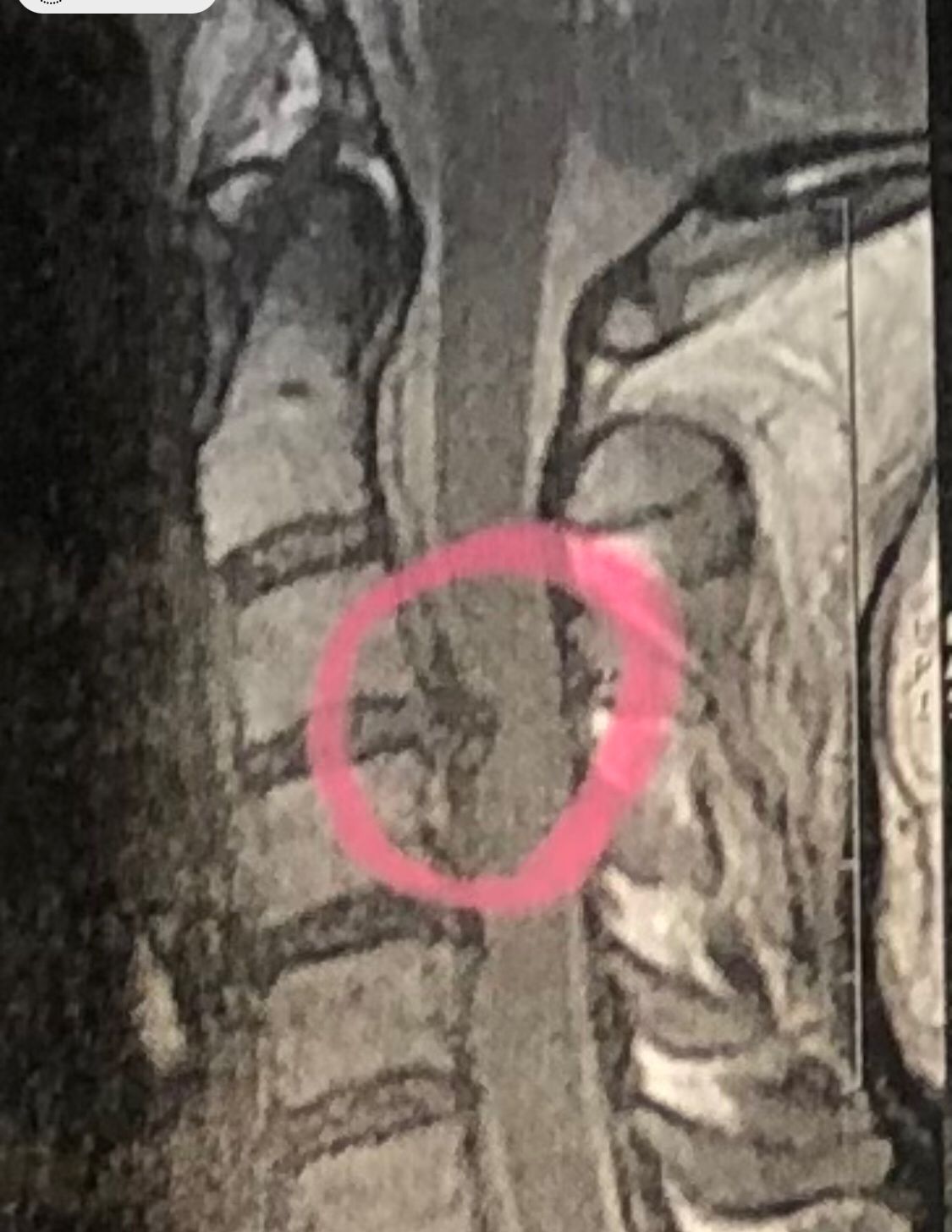
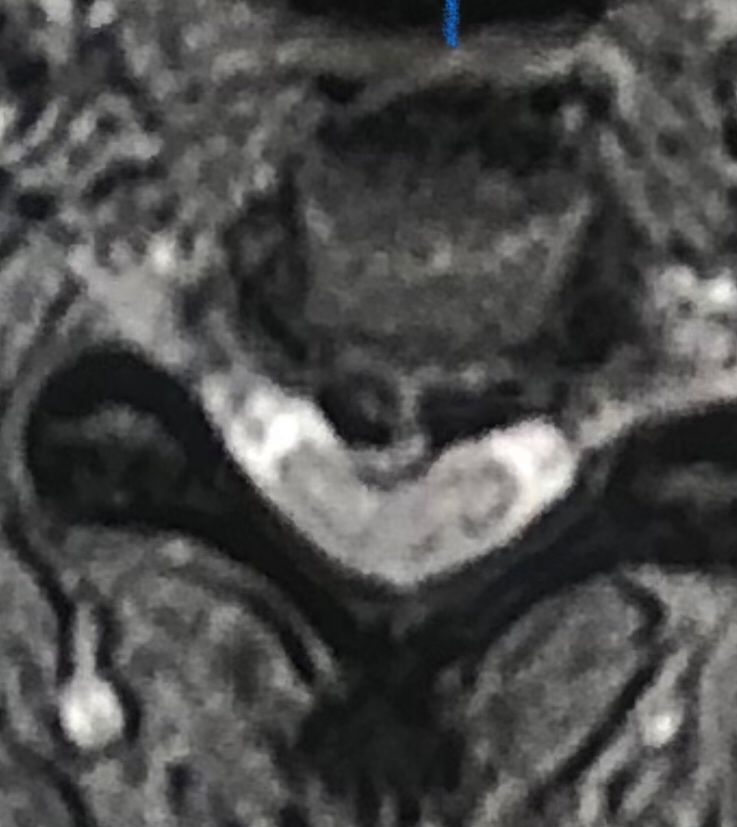
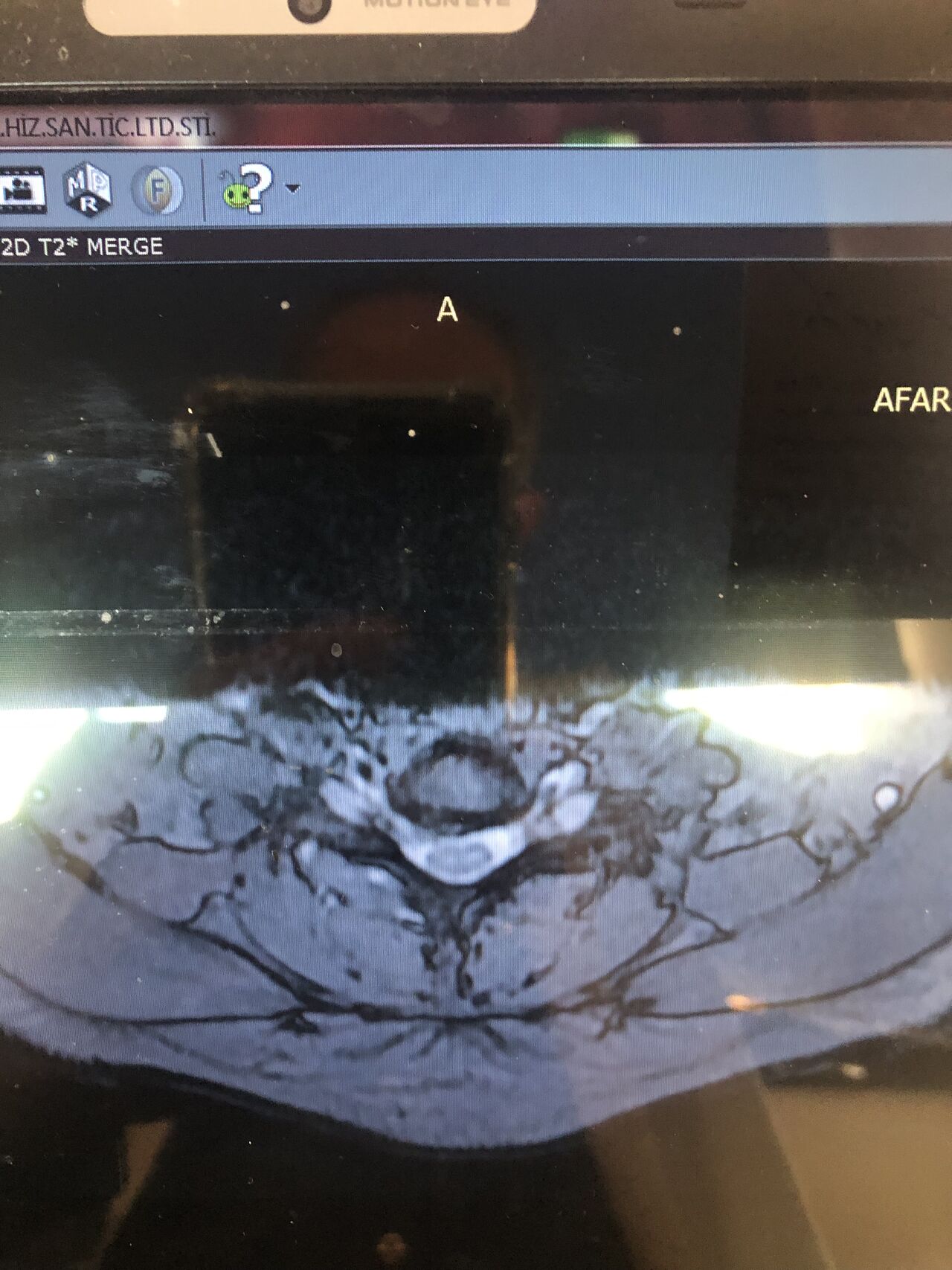
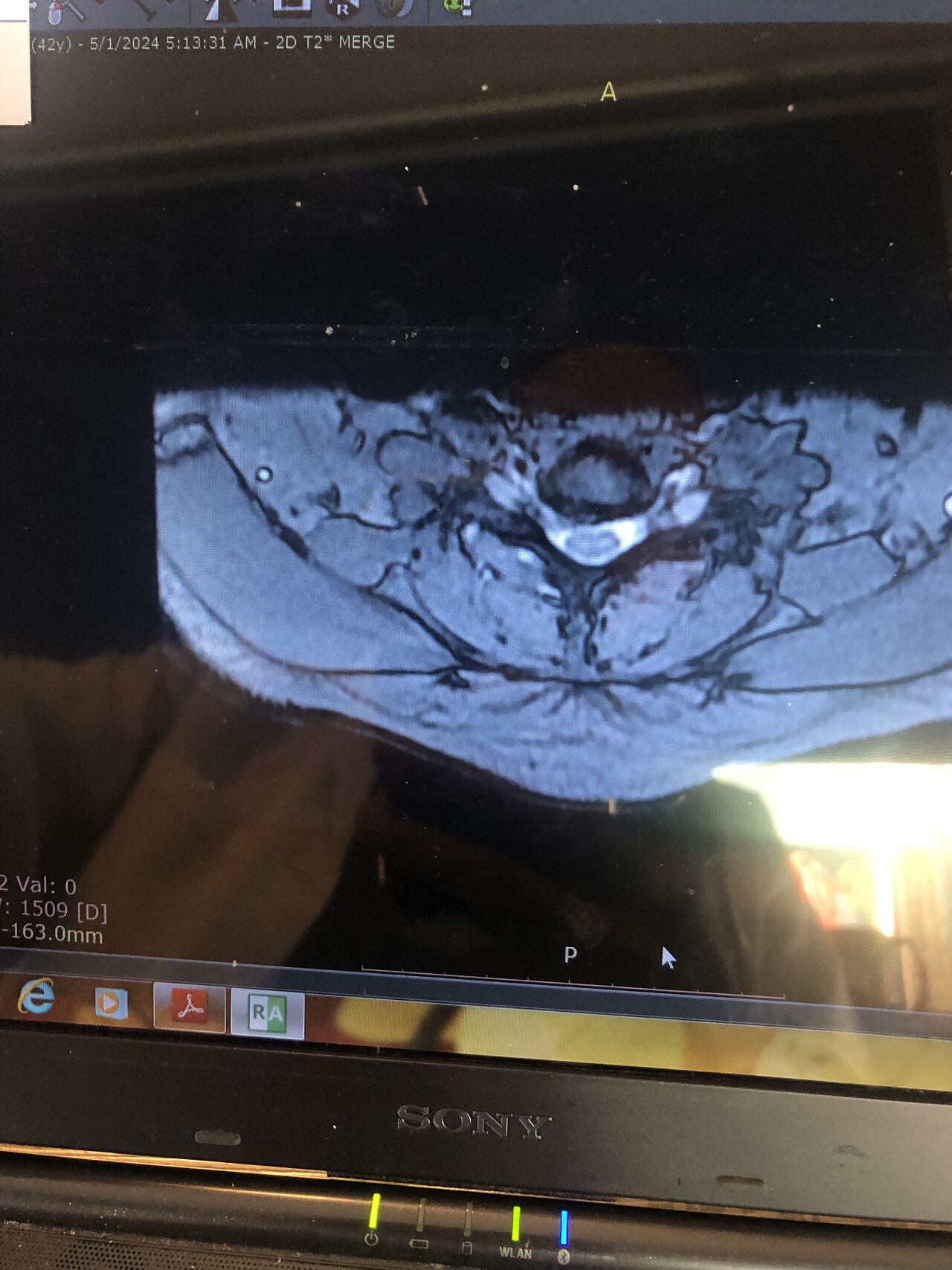
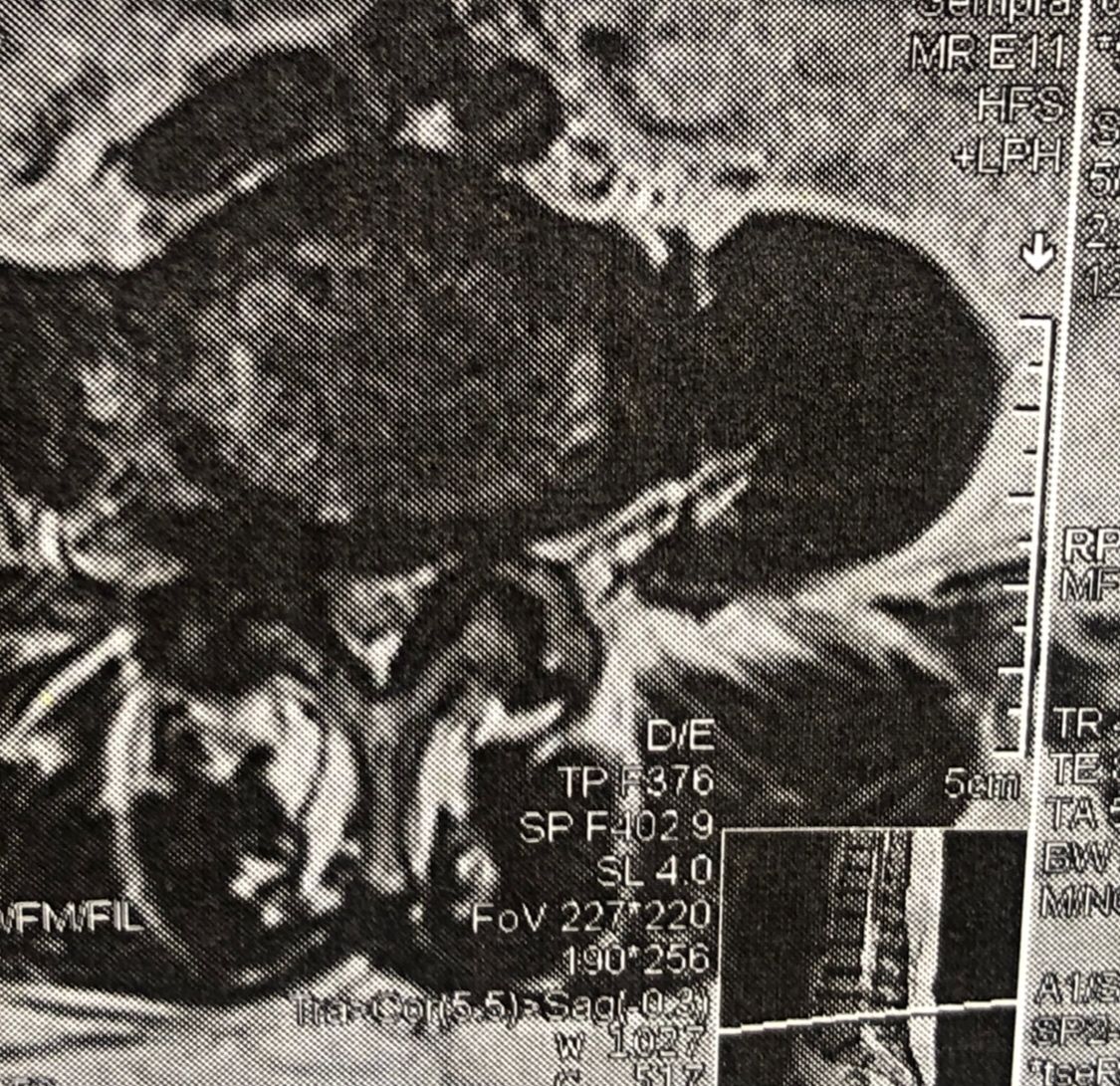
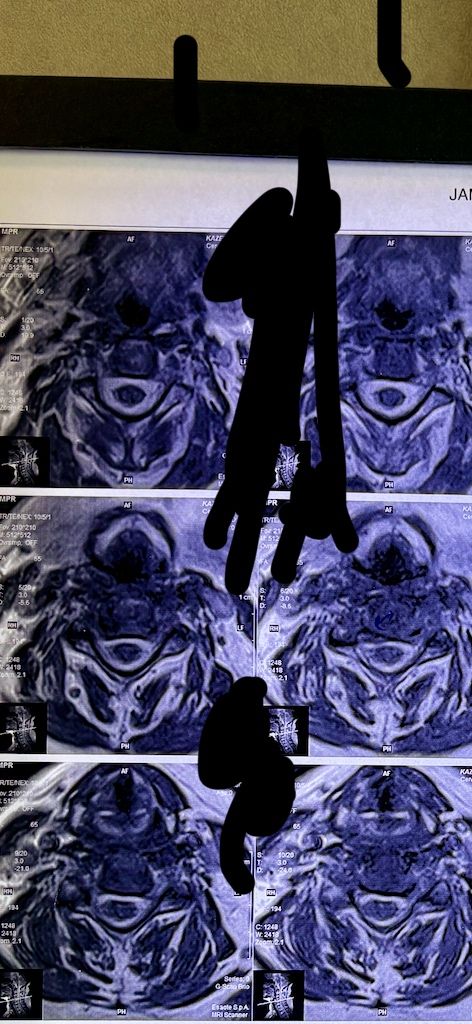
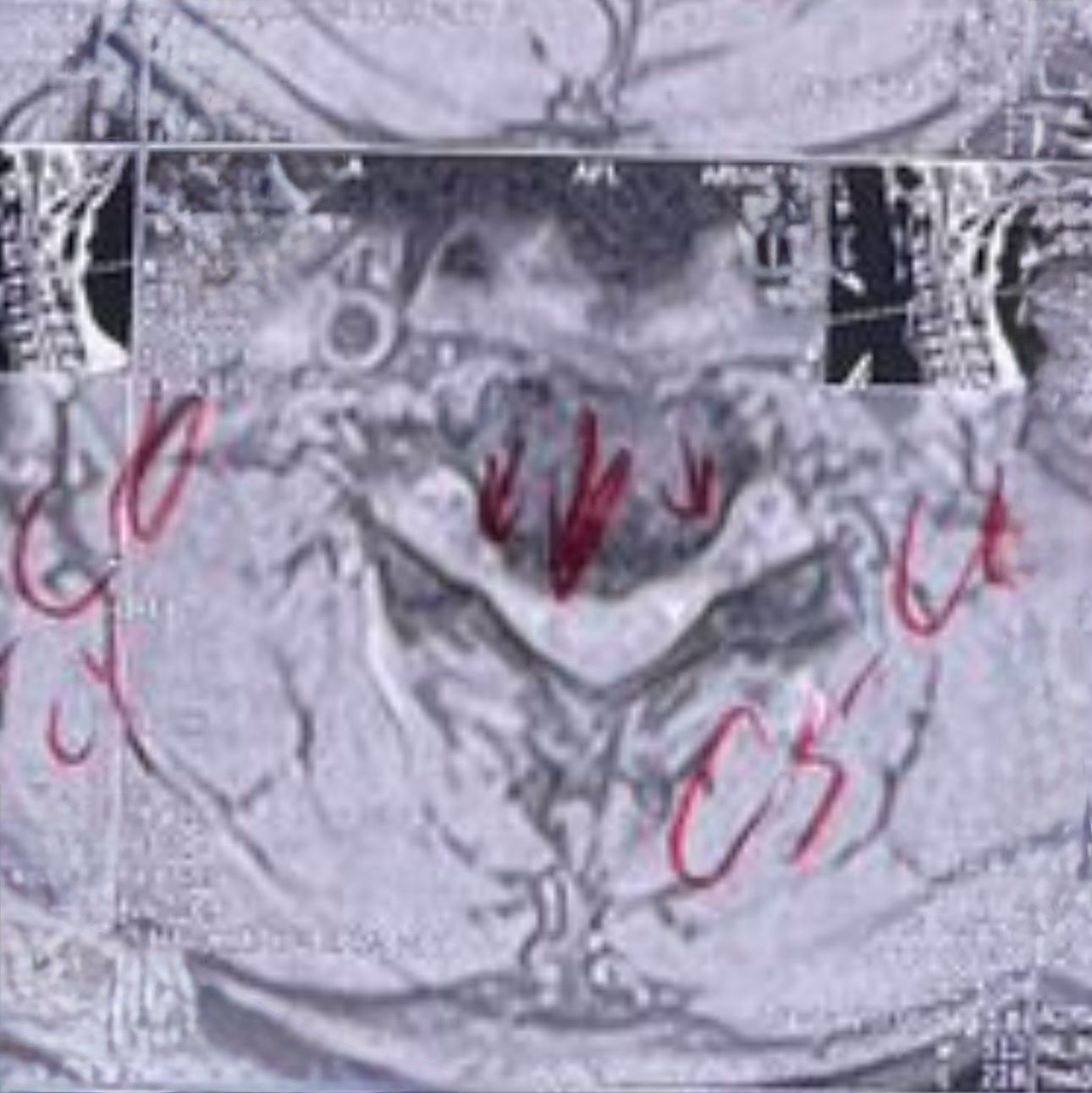
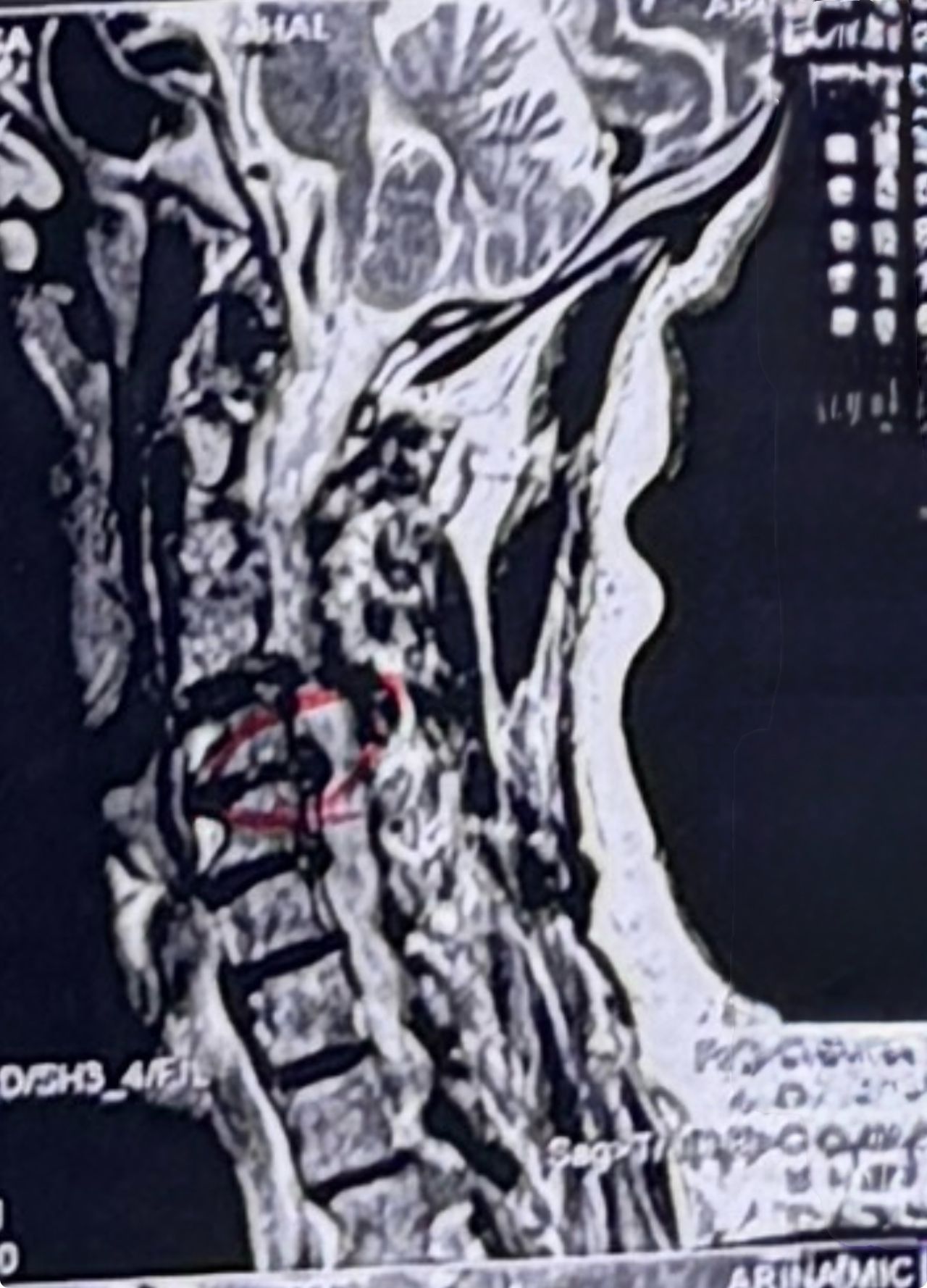
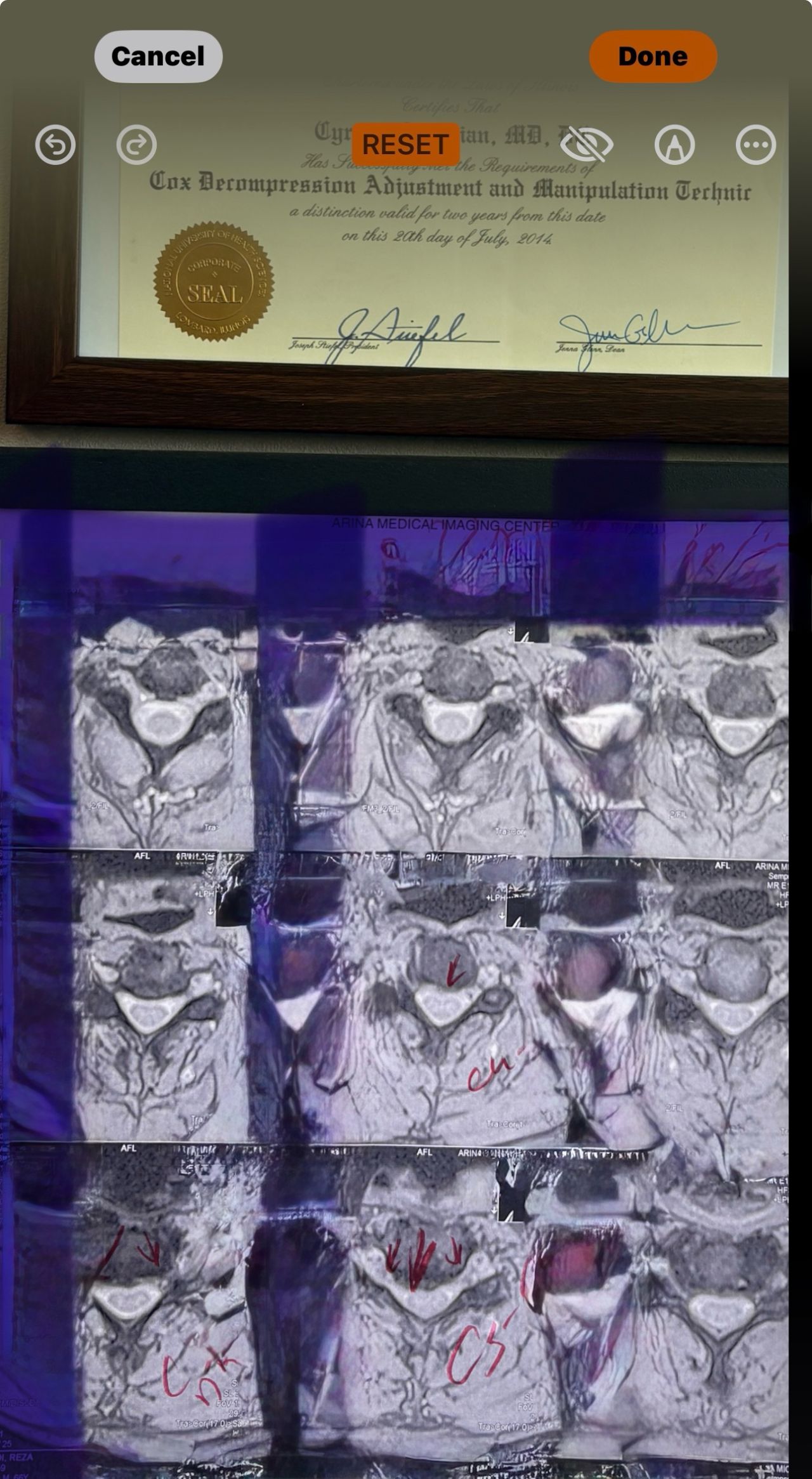
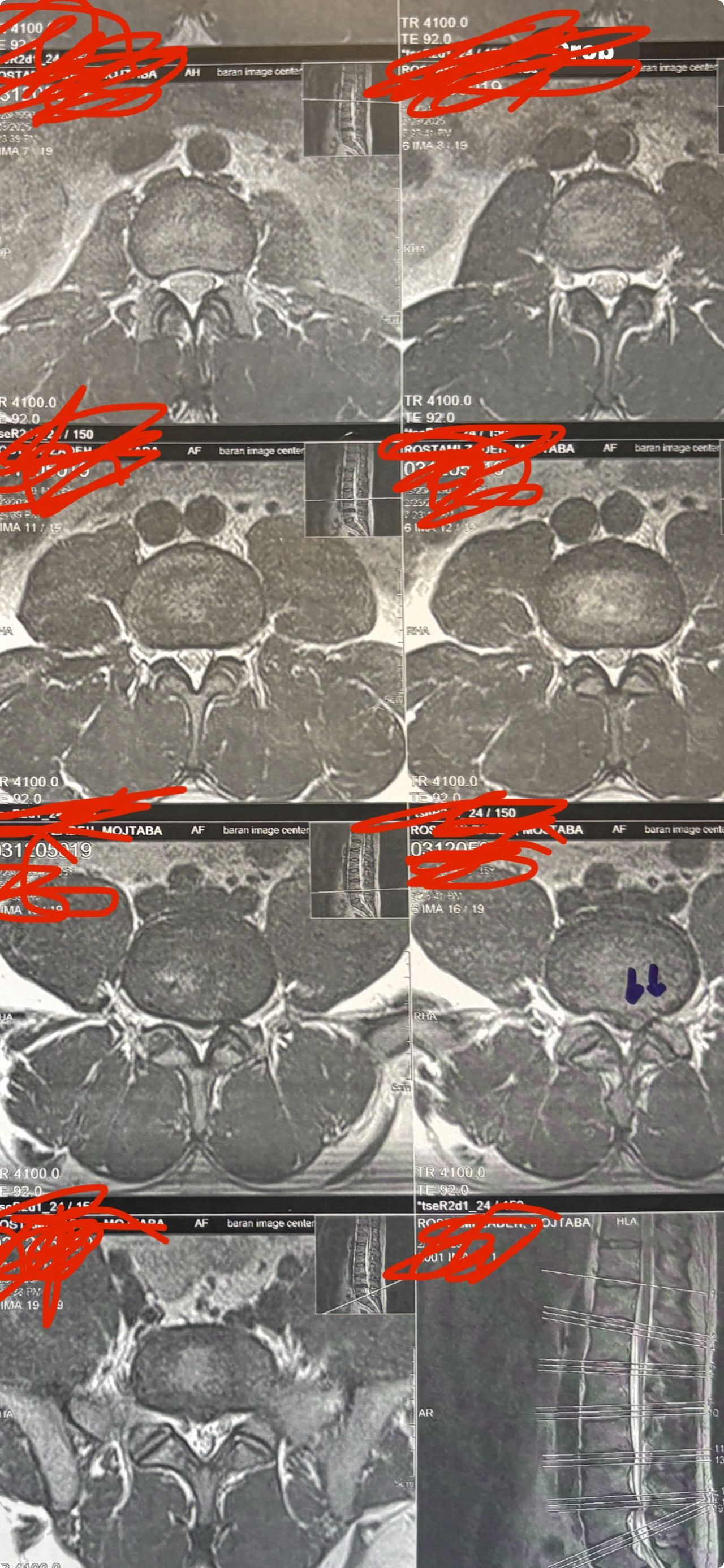
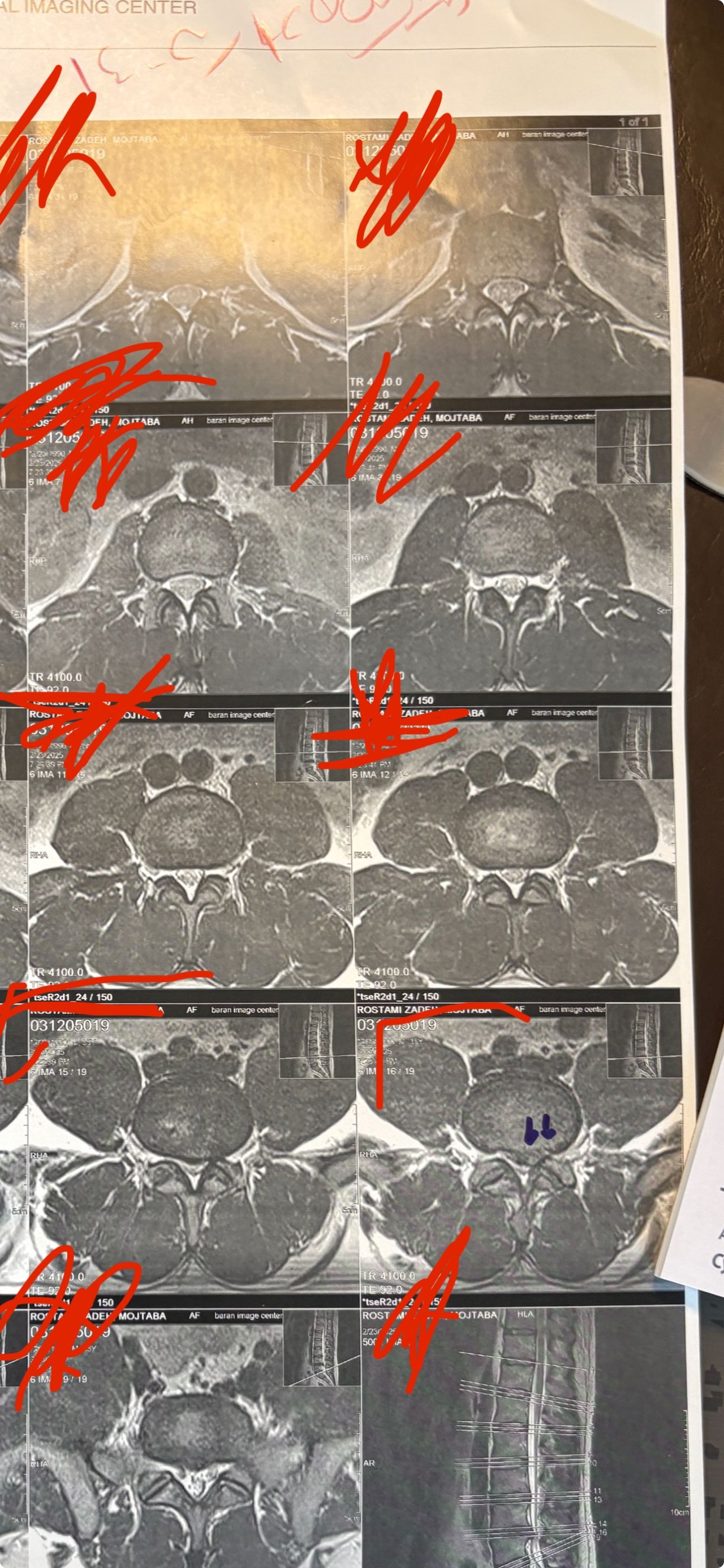
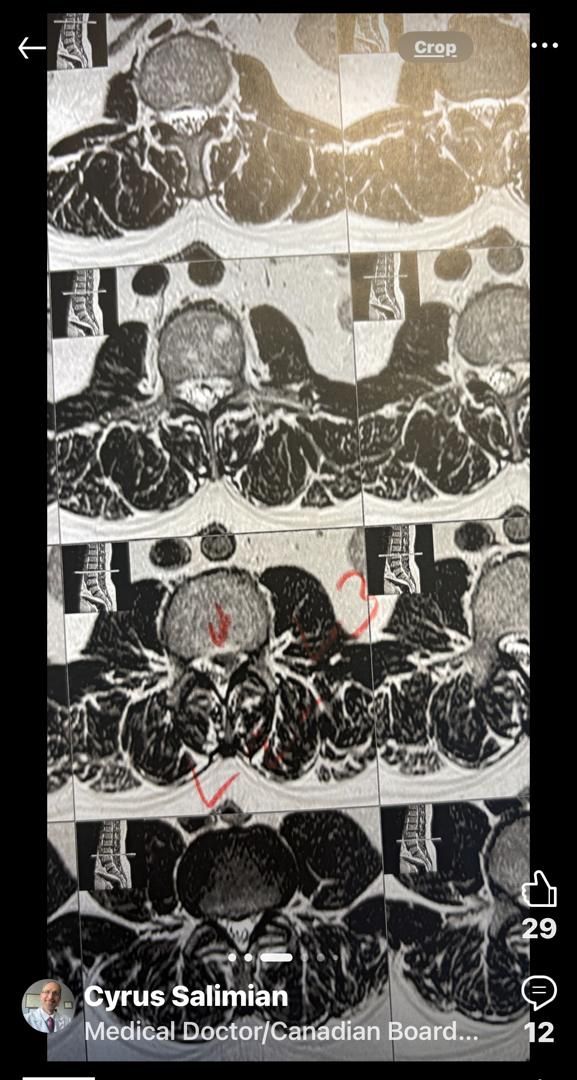
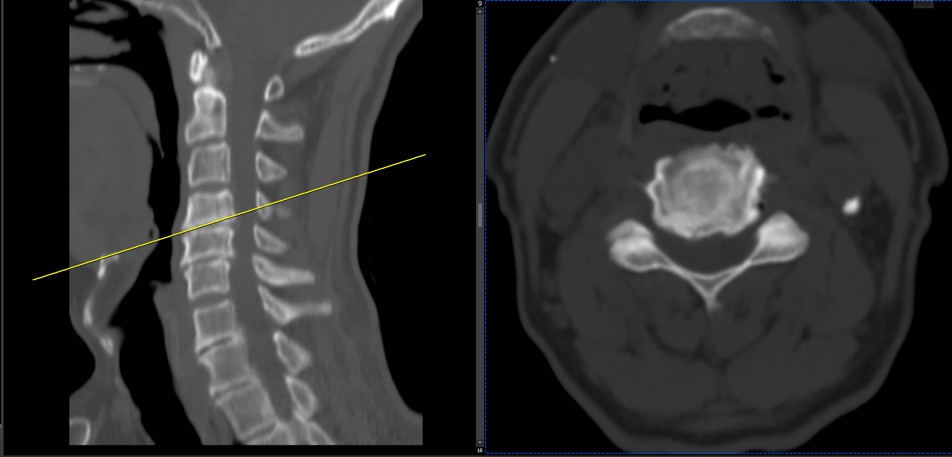
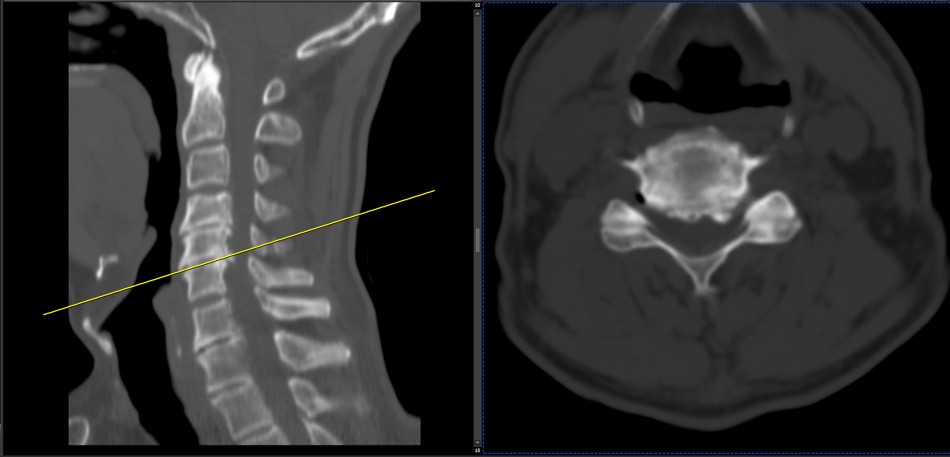
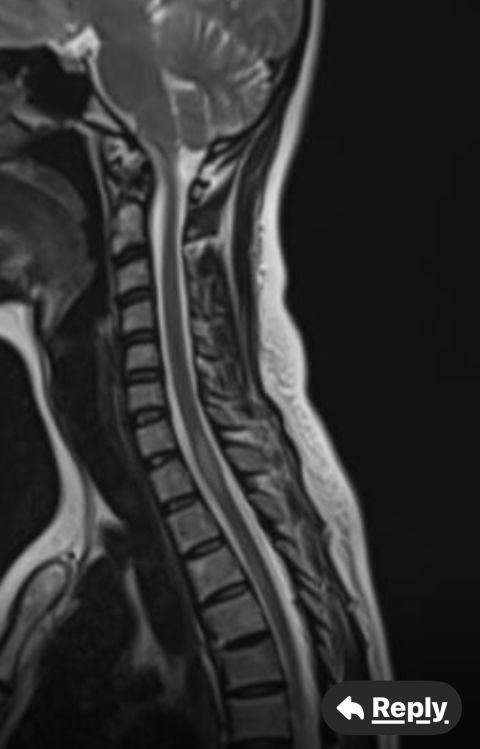
30 year old patient of mine with R. IVF disc extrusion of C 5-6 with R upper extremity pain and numbness without neurological deficit was suggested to have urgent surgery
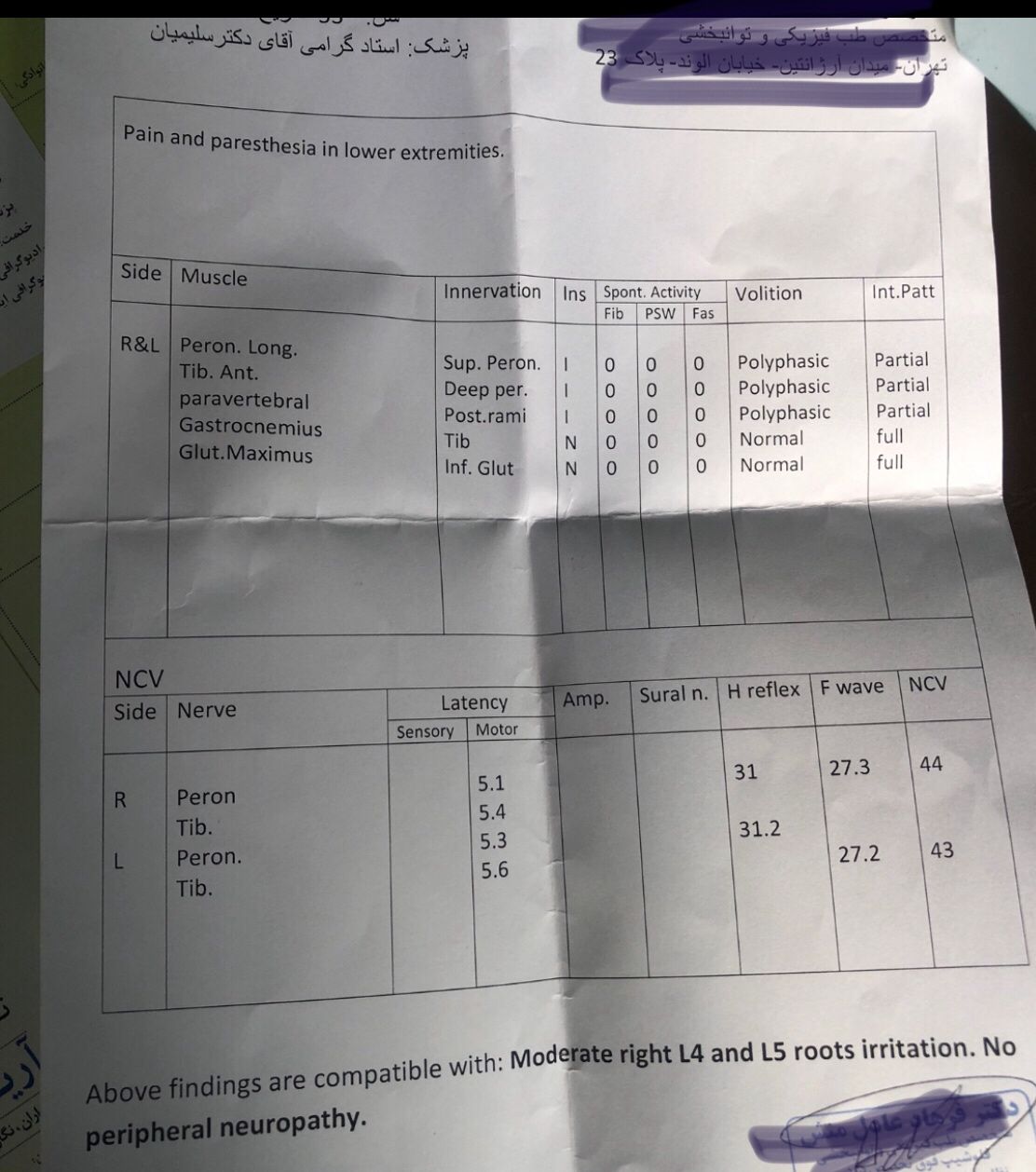
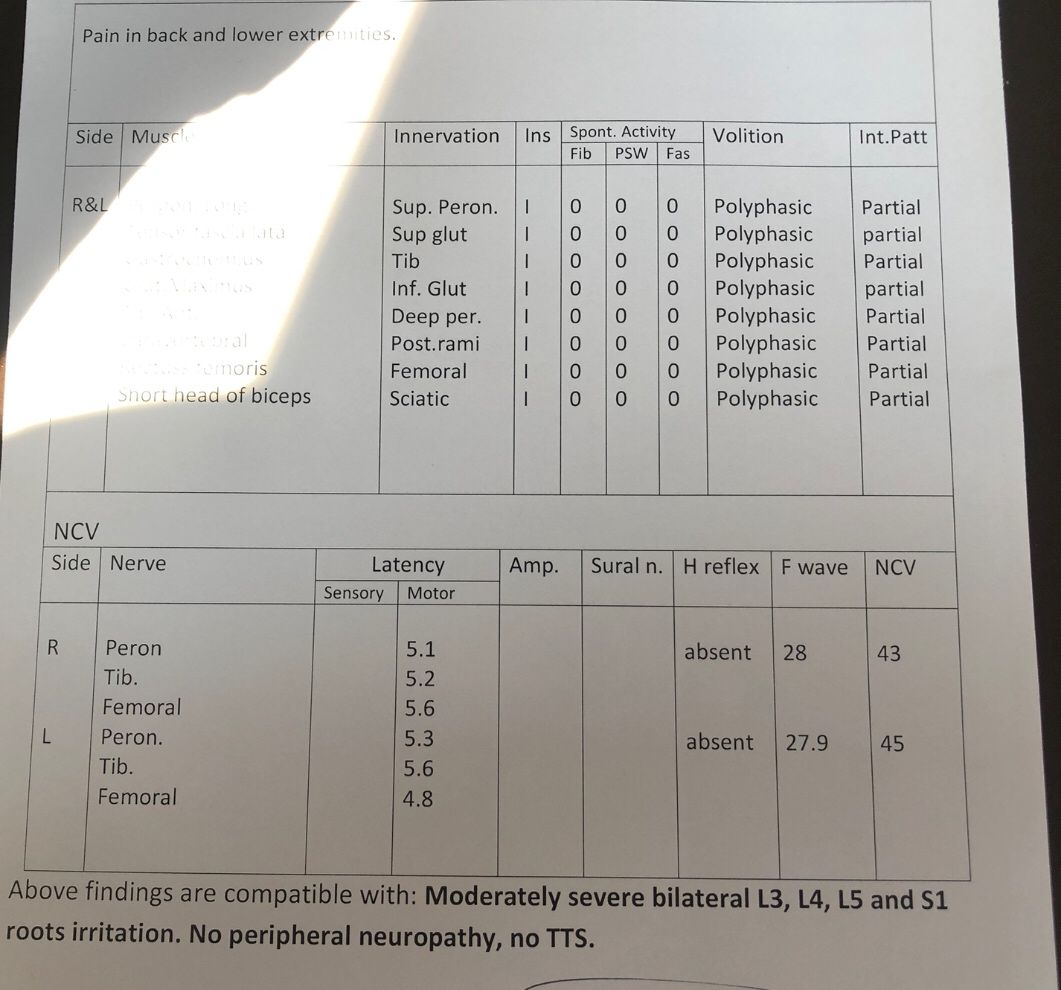
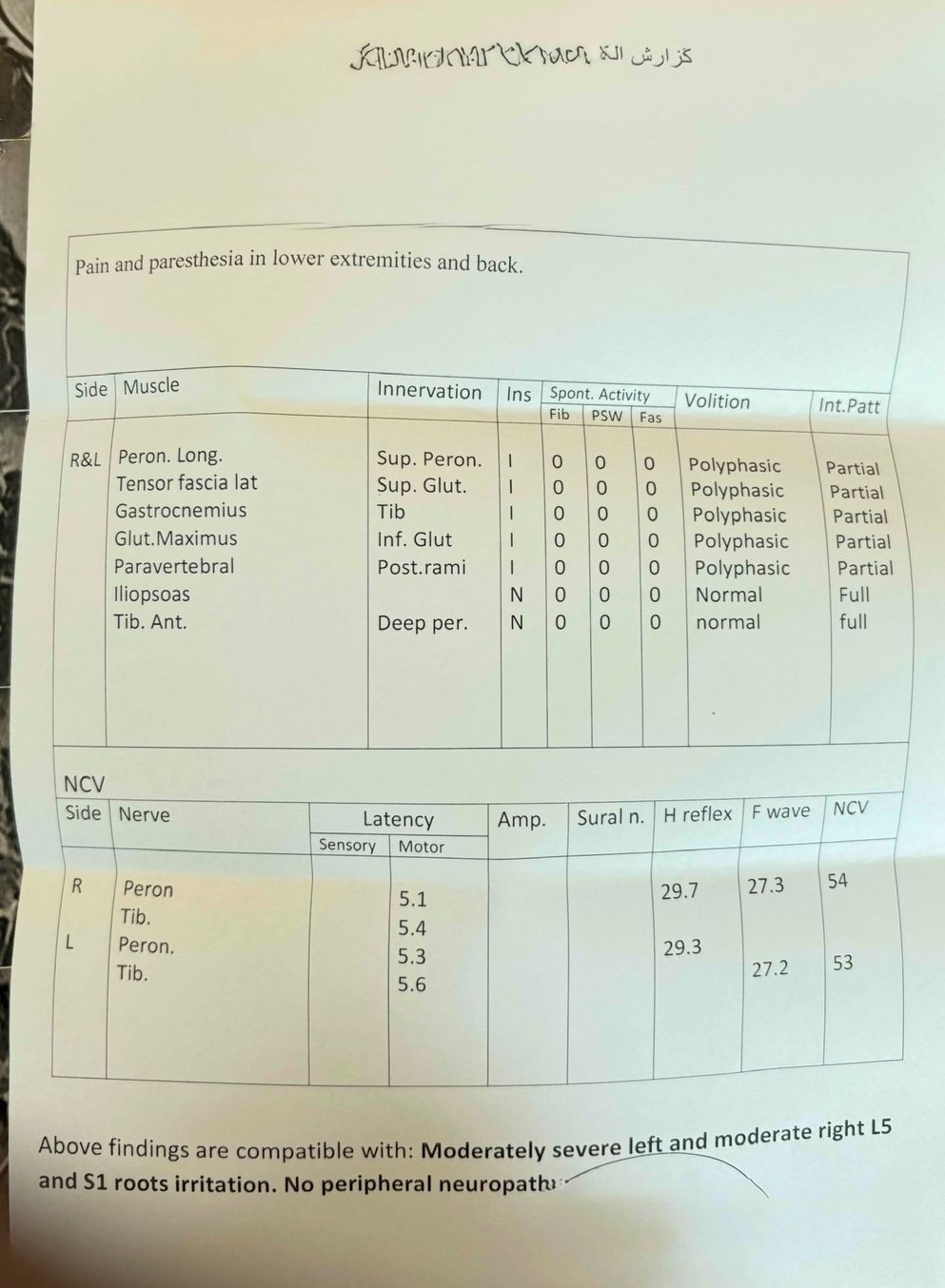
in his EMG. NCV didn’t have any active axonal loss

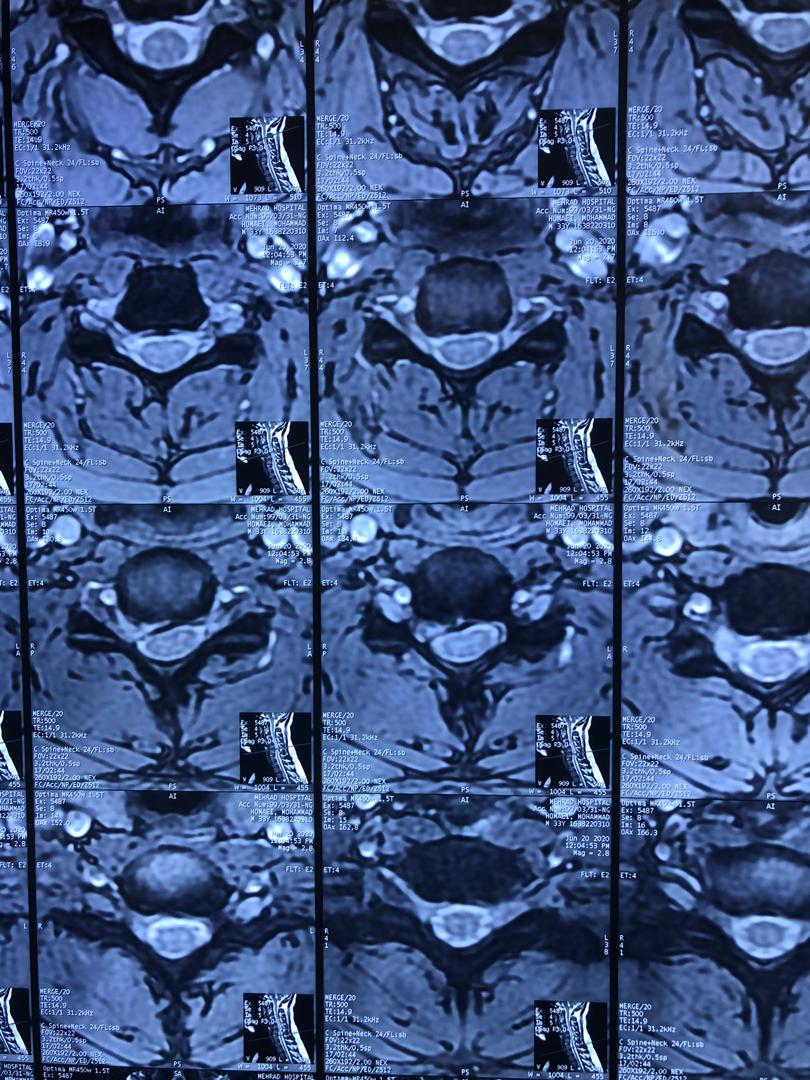
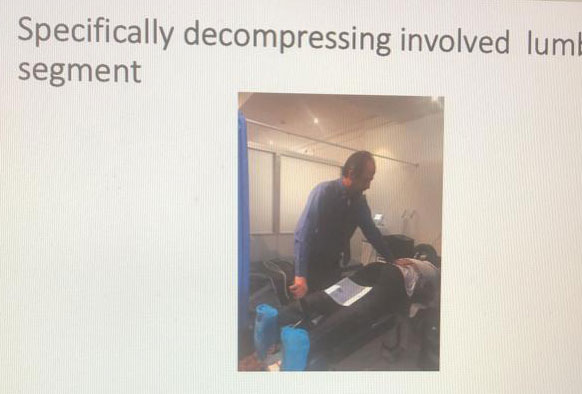
got 20 sessions of chiropractic care in one month by me mainly using decompression and C0-C1 prone drop manipulation and 3 sessions of mild adjustment to segments above disc herniation. No direct adjustment to the involved disc extrusion

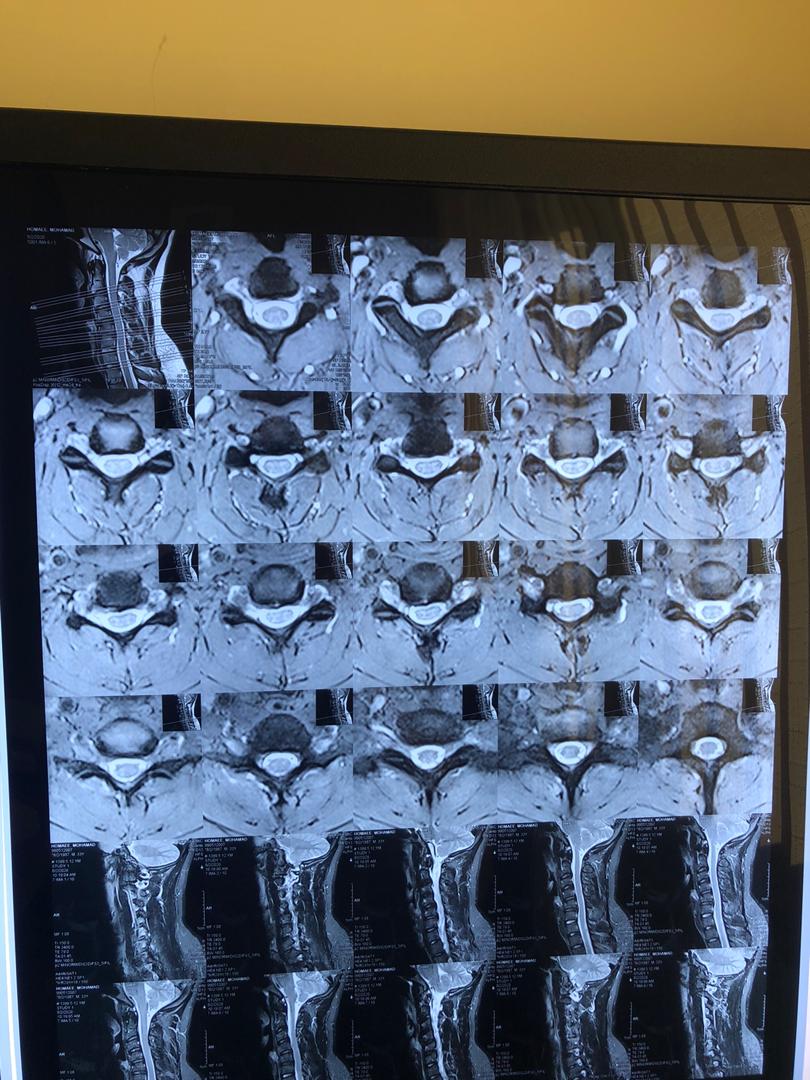
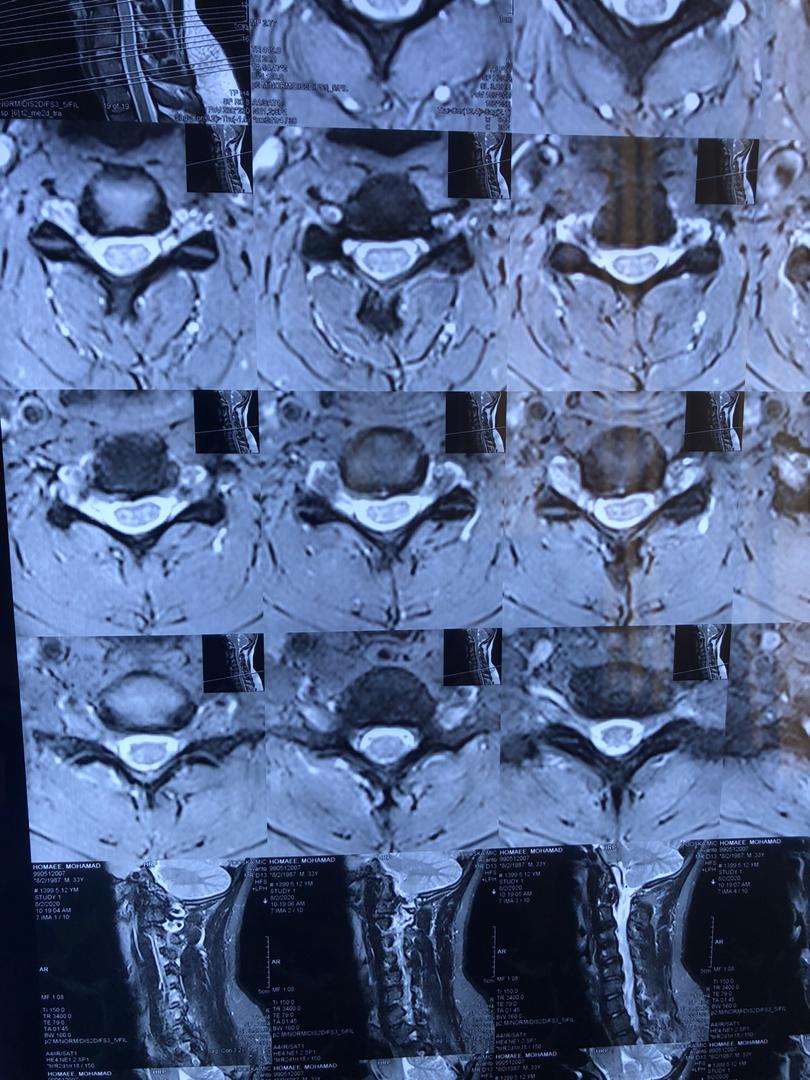
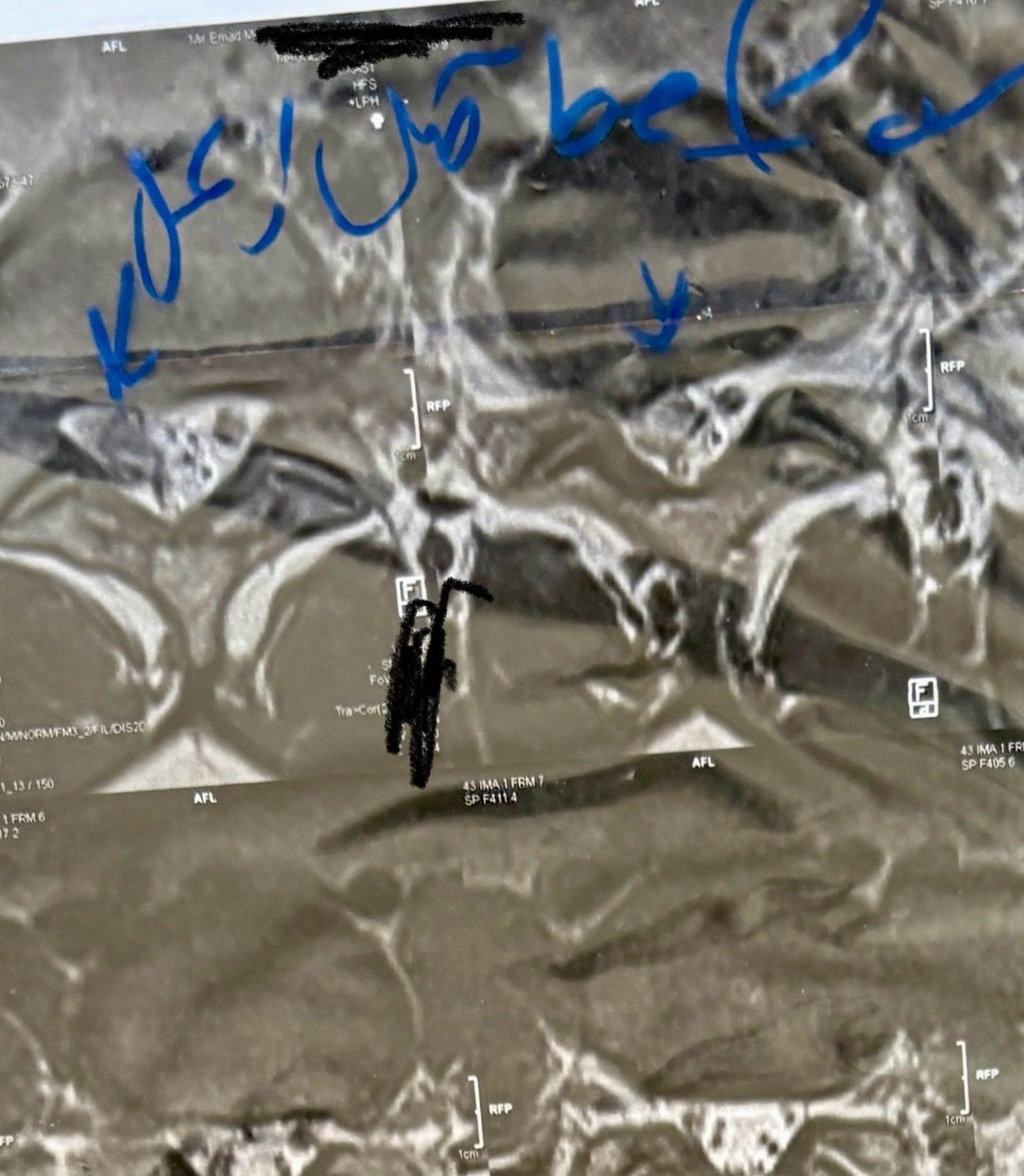
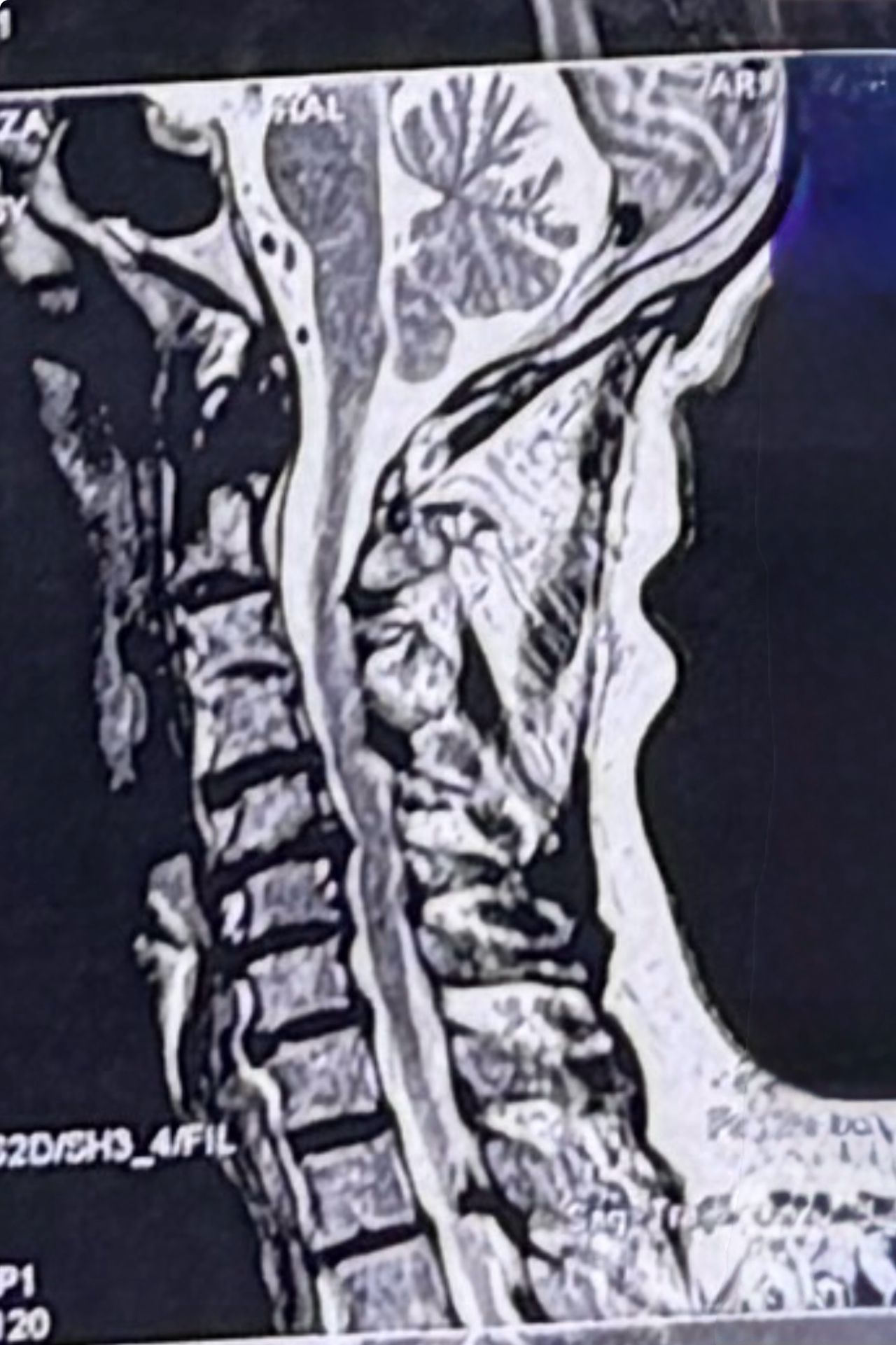
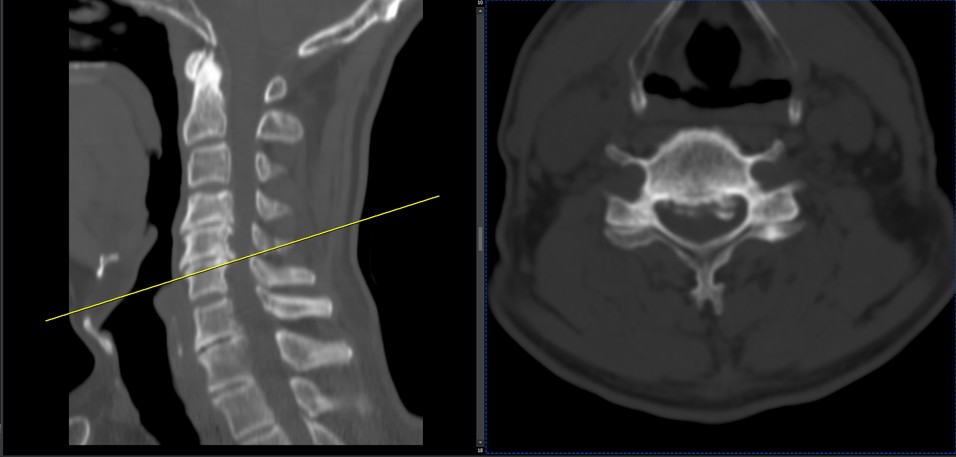
After treatment:
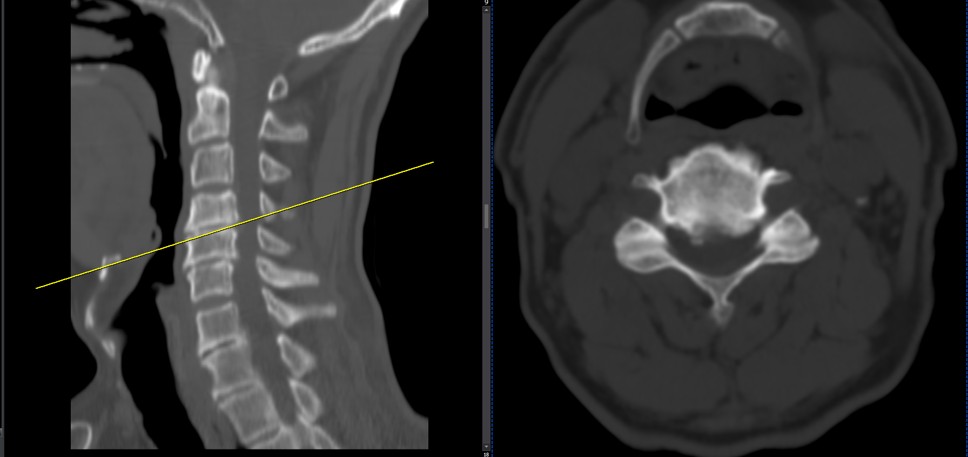
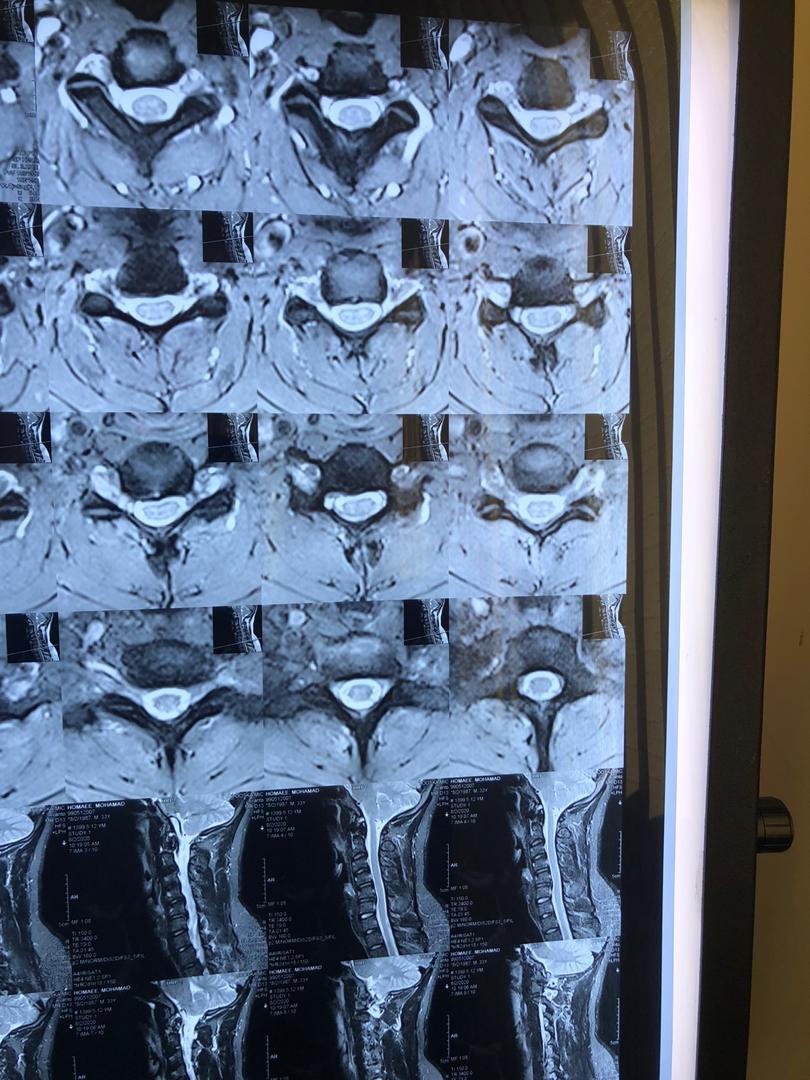
reduction of R. IVFdisc extrusion by more than 50%.
90% improvement in patient’s signs and symptoms and preventing of unnecessary expensive surgery
following one month of cervical chiropractic spinal treatments


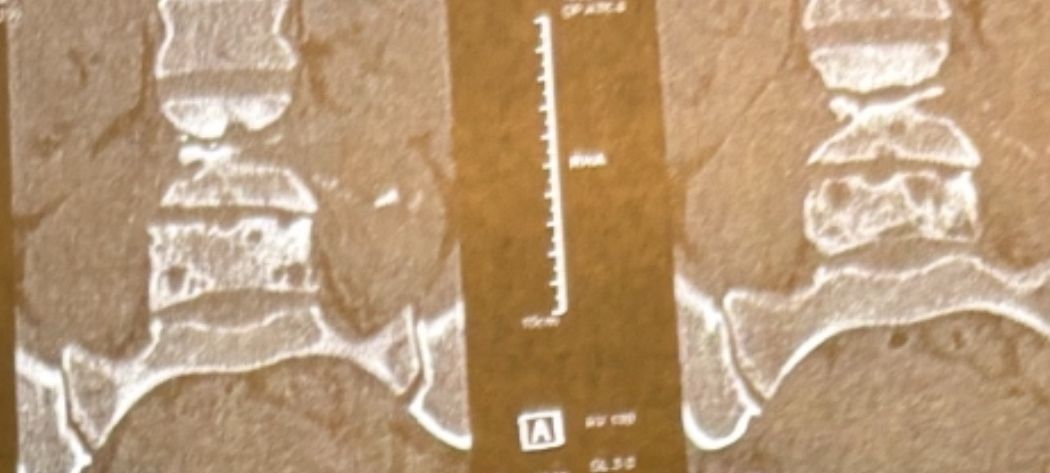
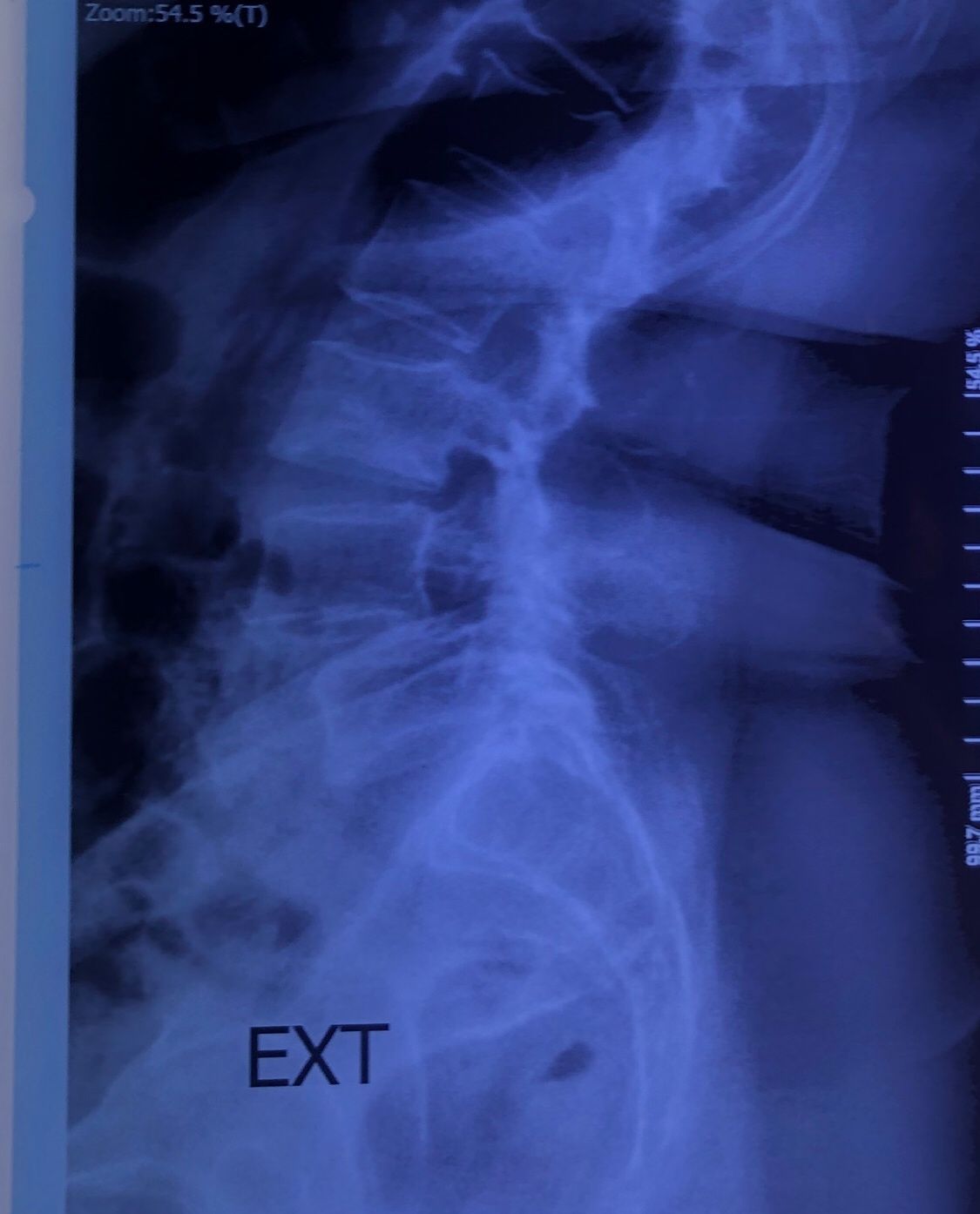
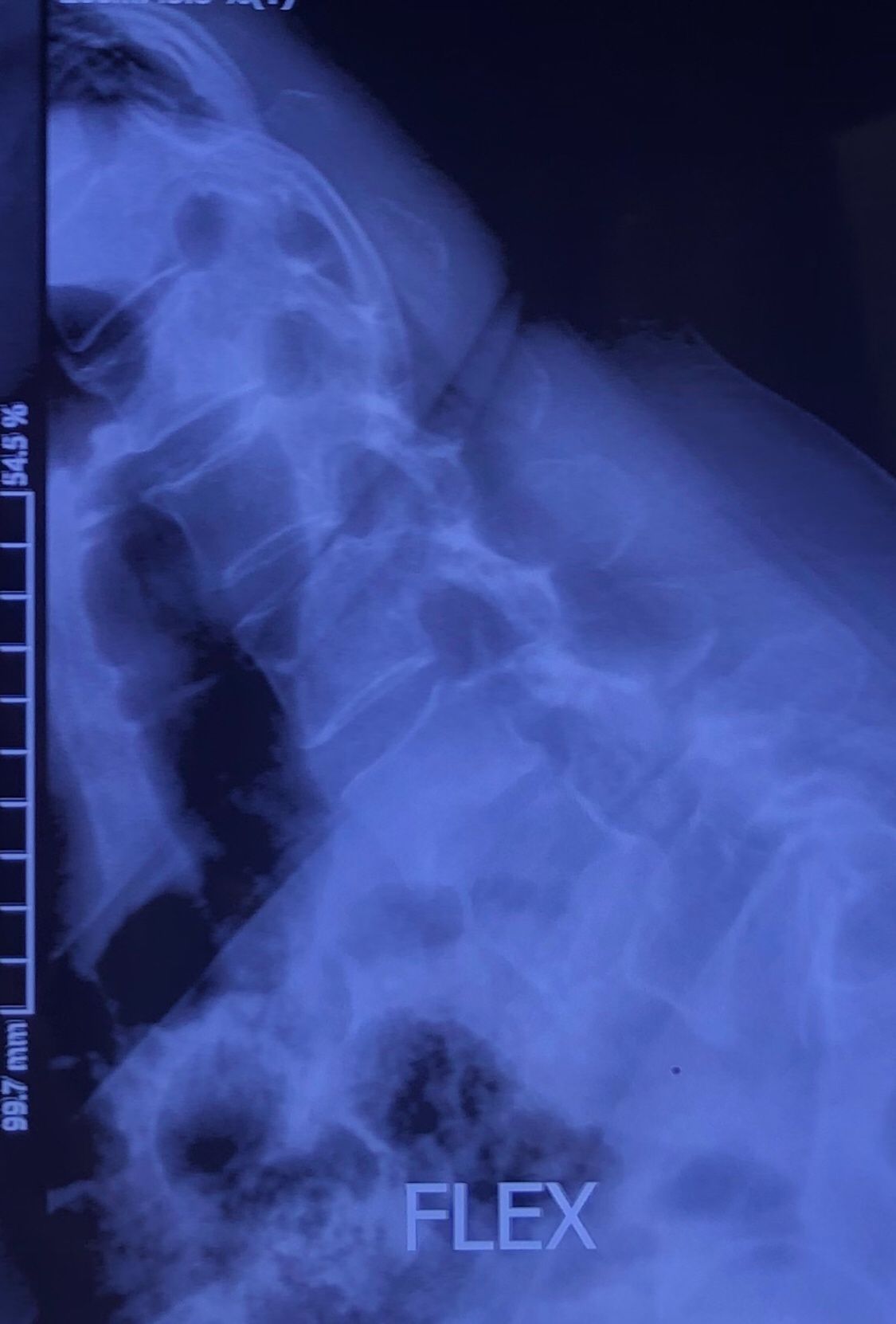
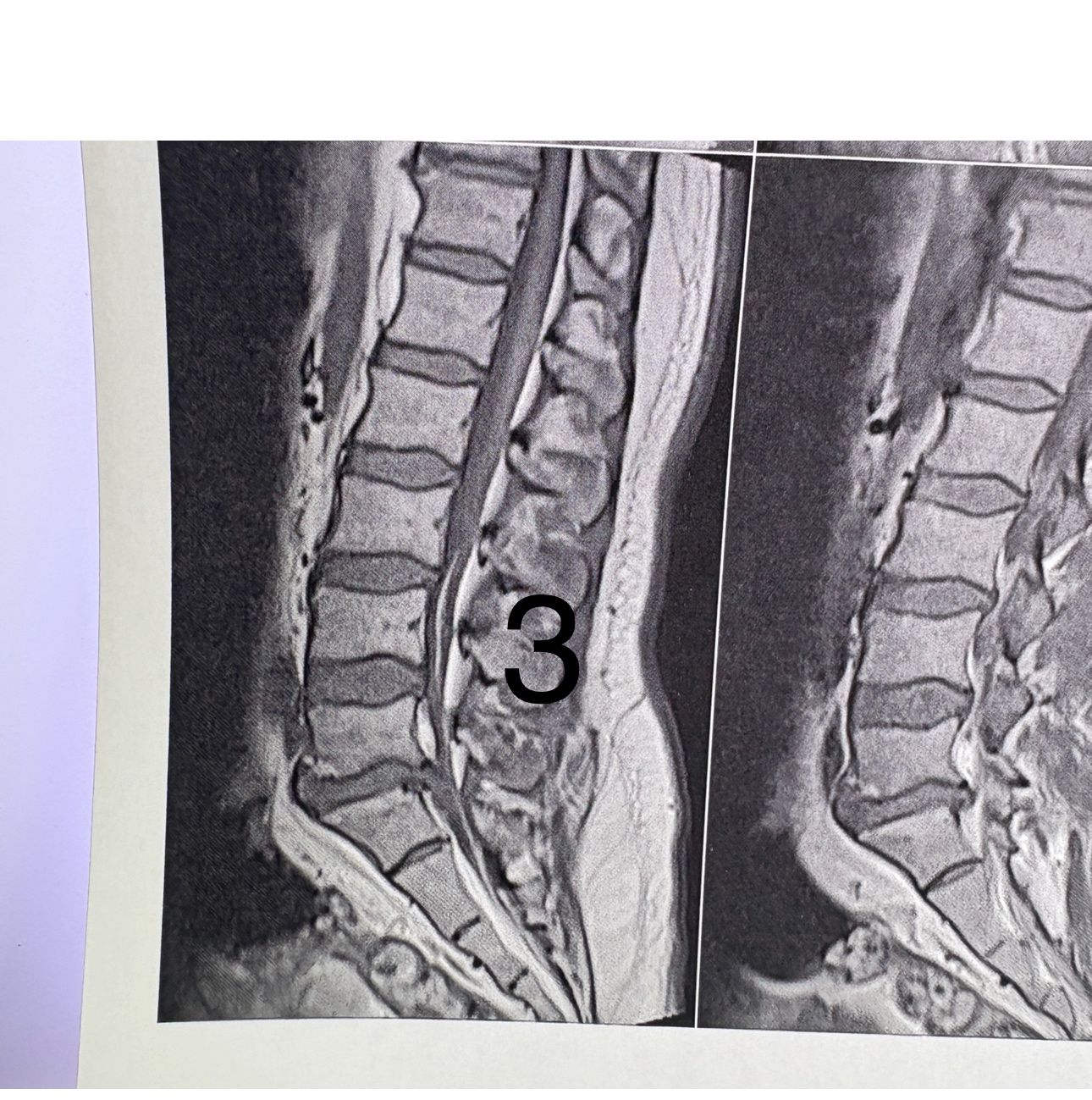
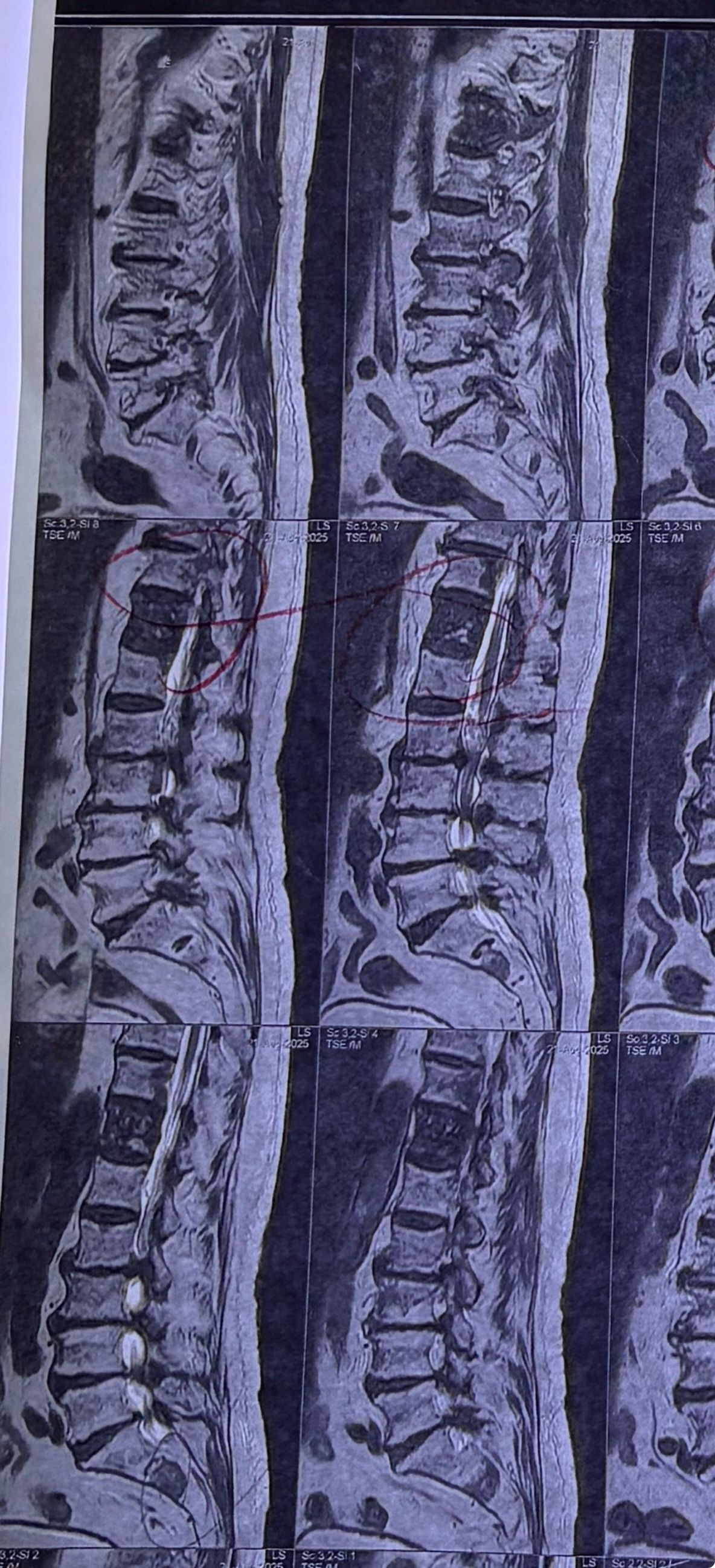
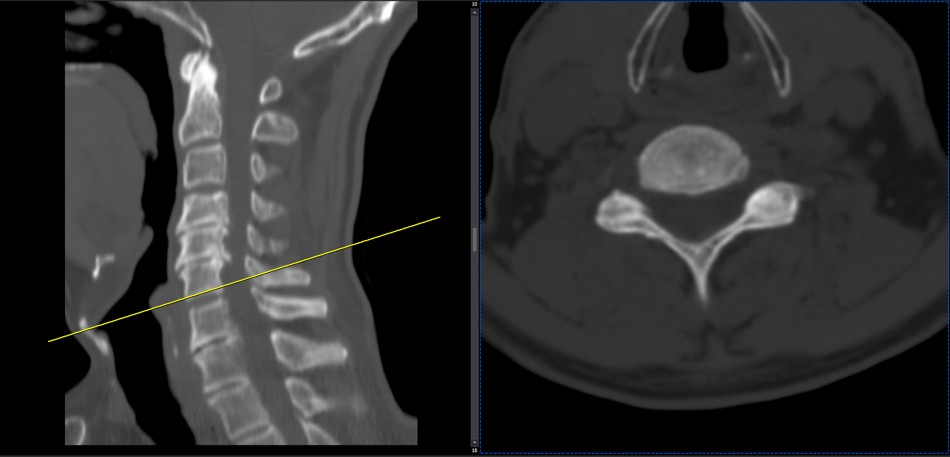
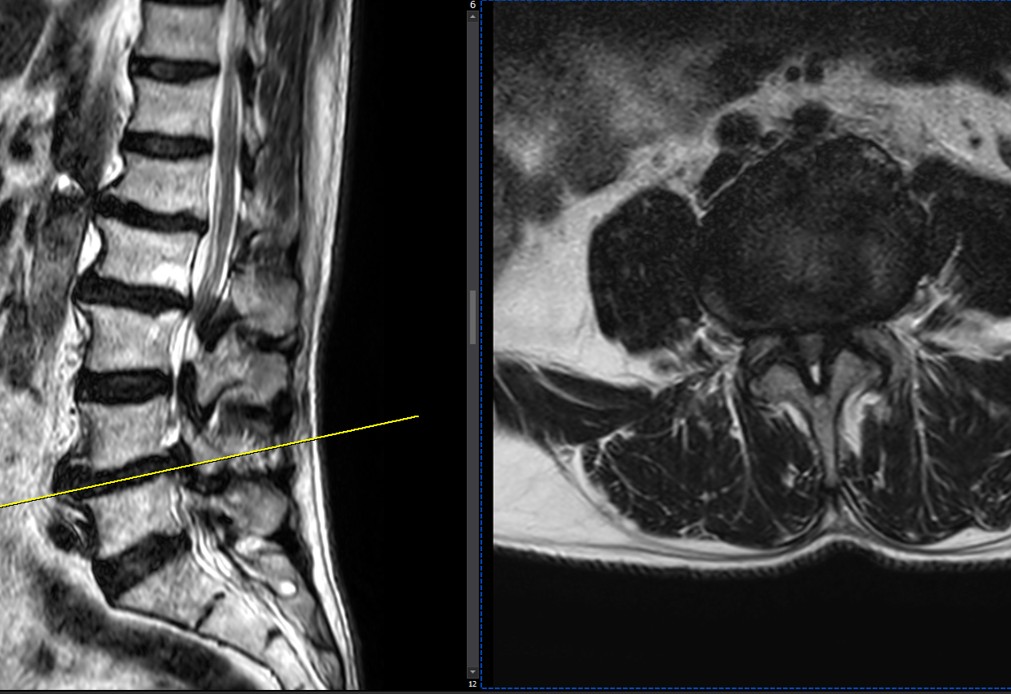
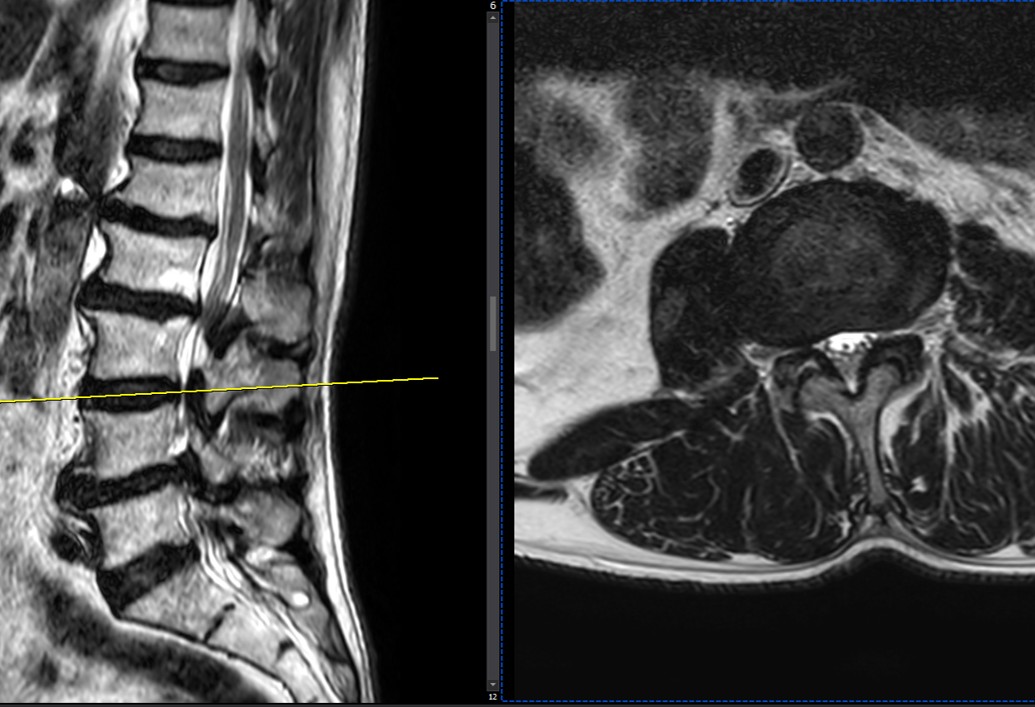
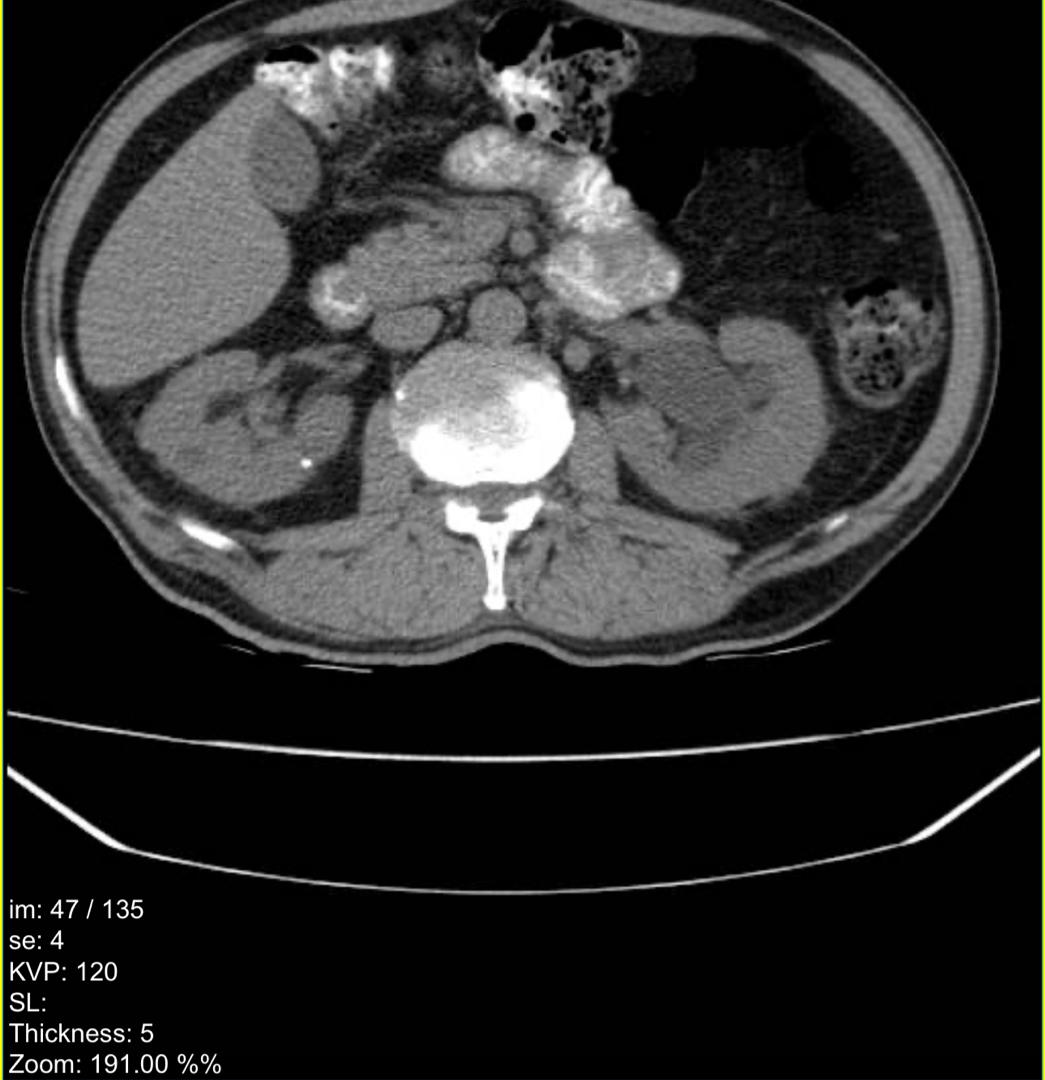
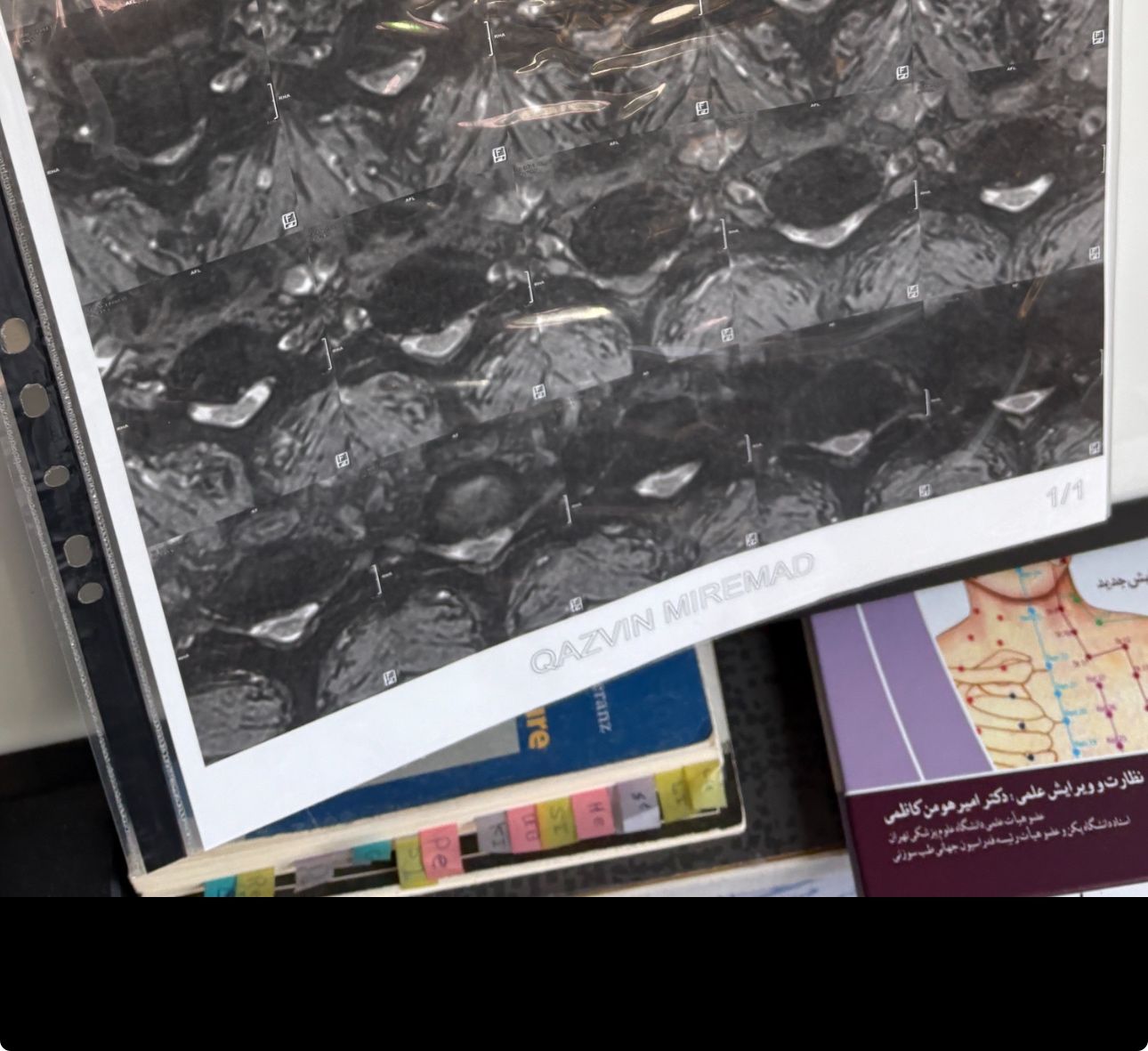
Case 3
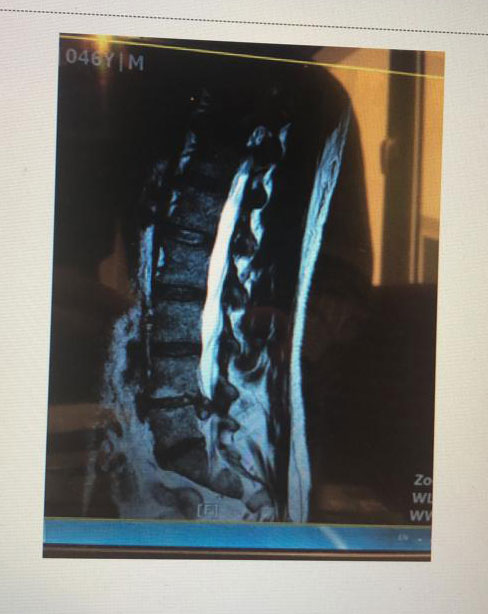
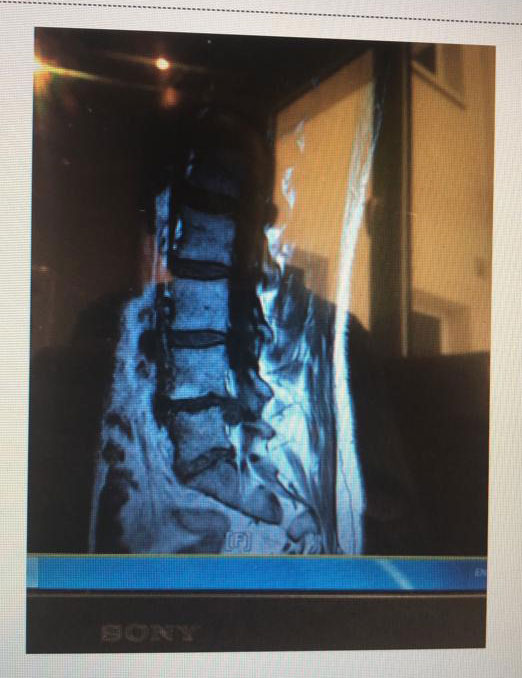


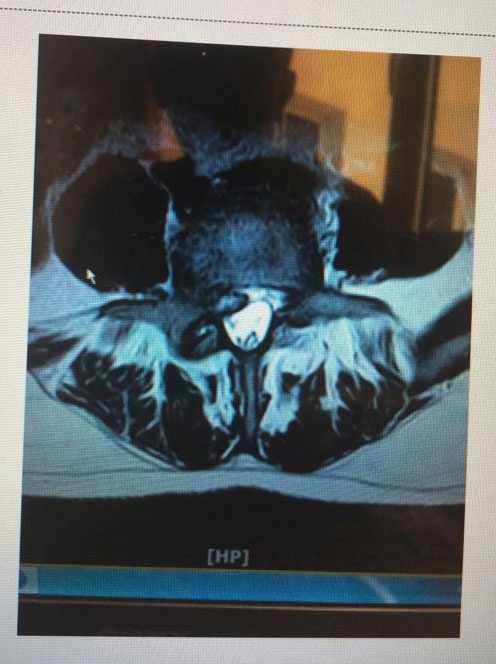


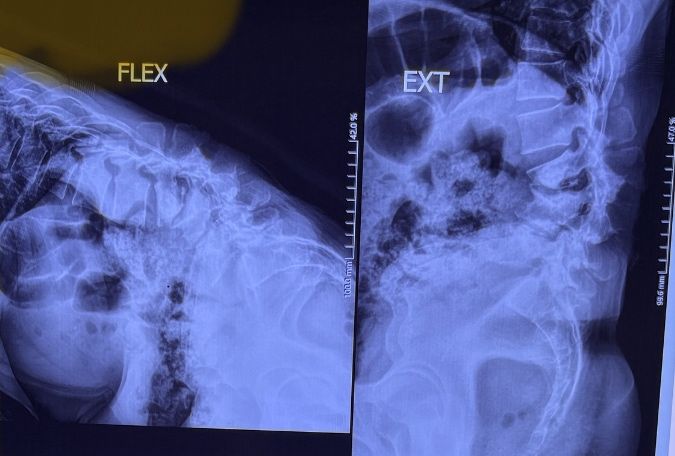
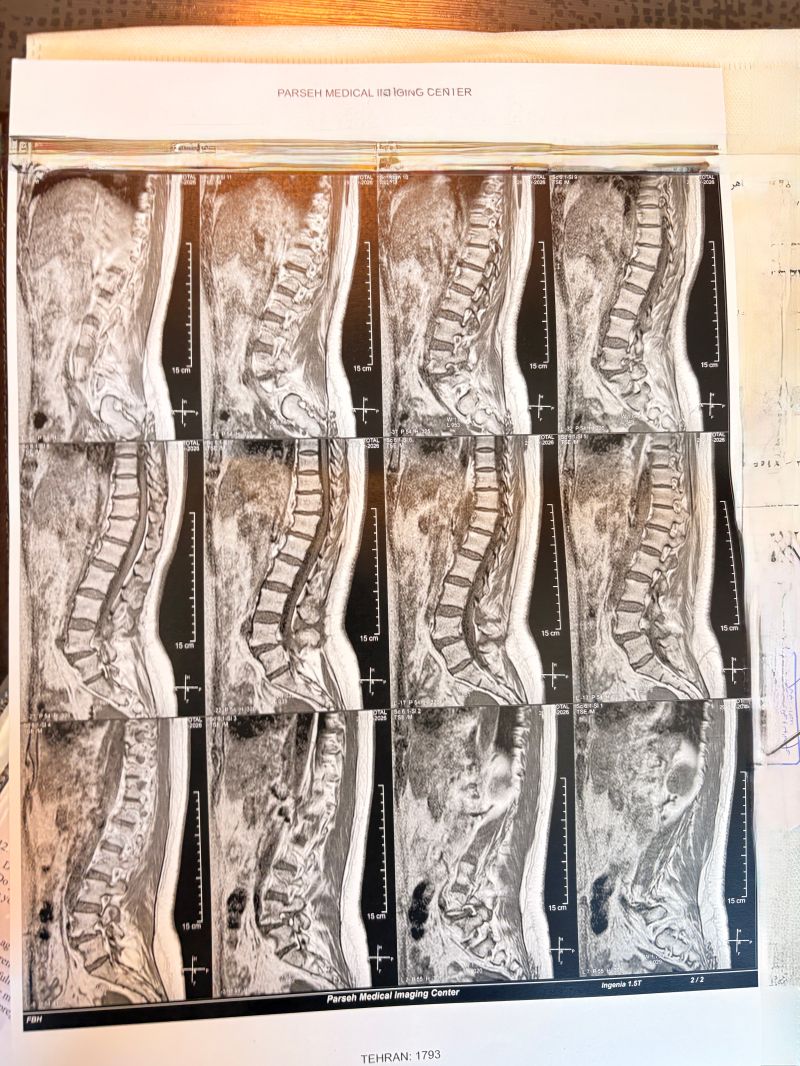
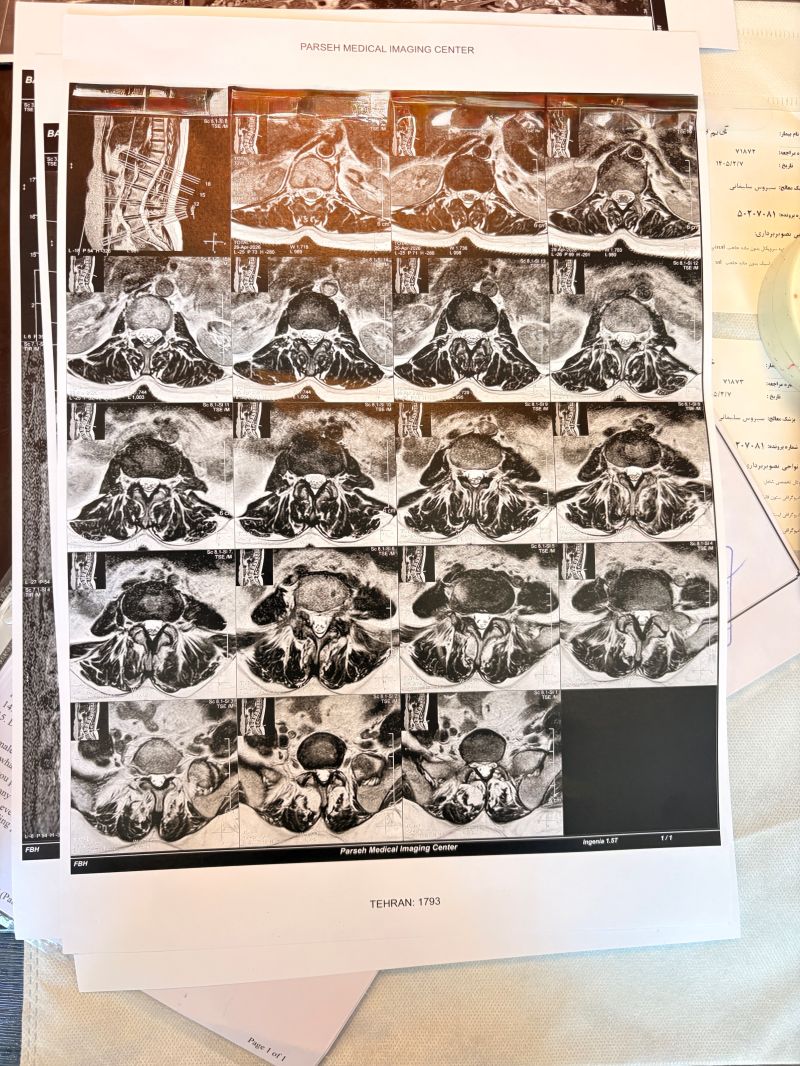
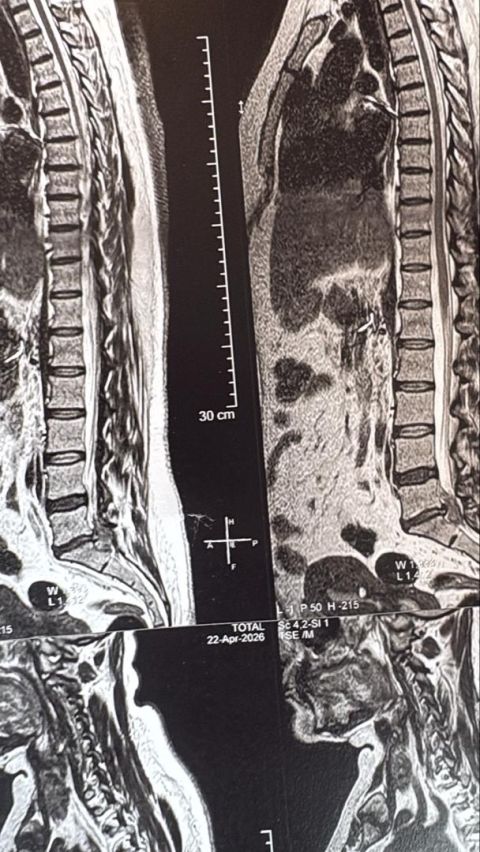
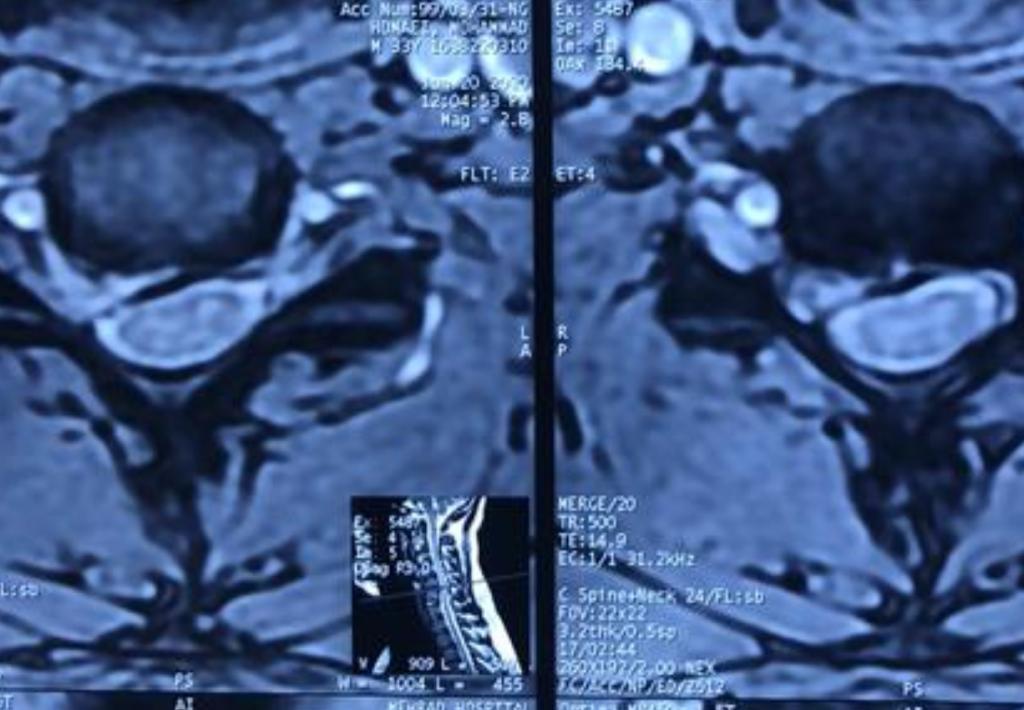
Case 4
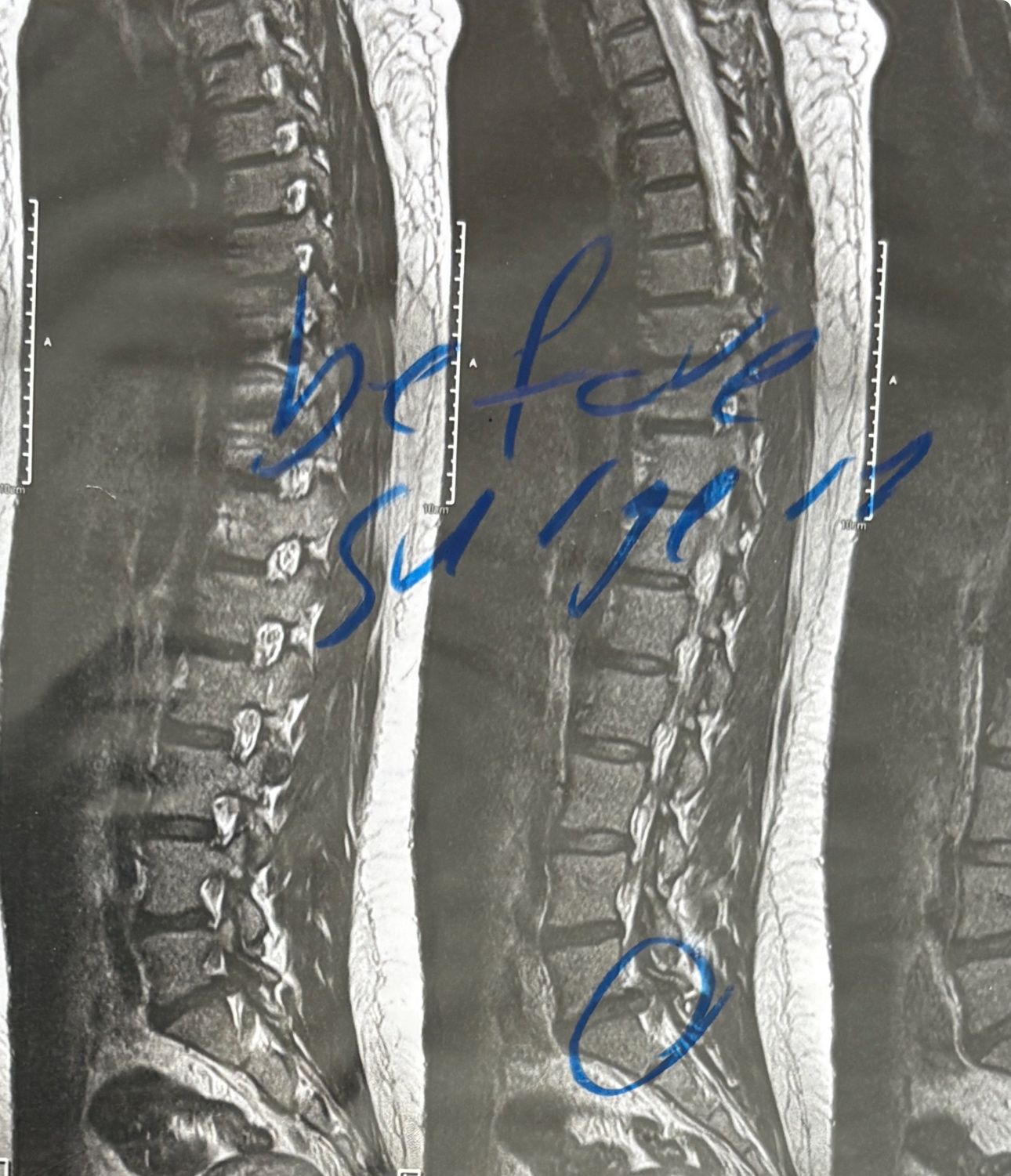
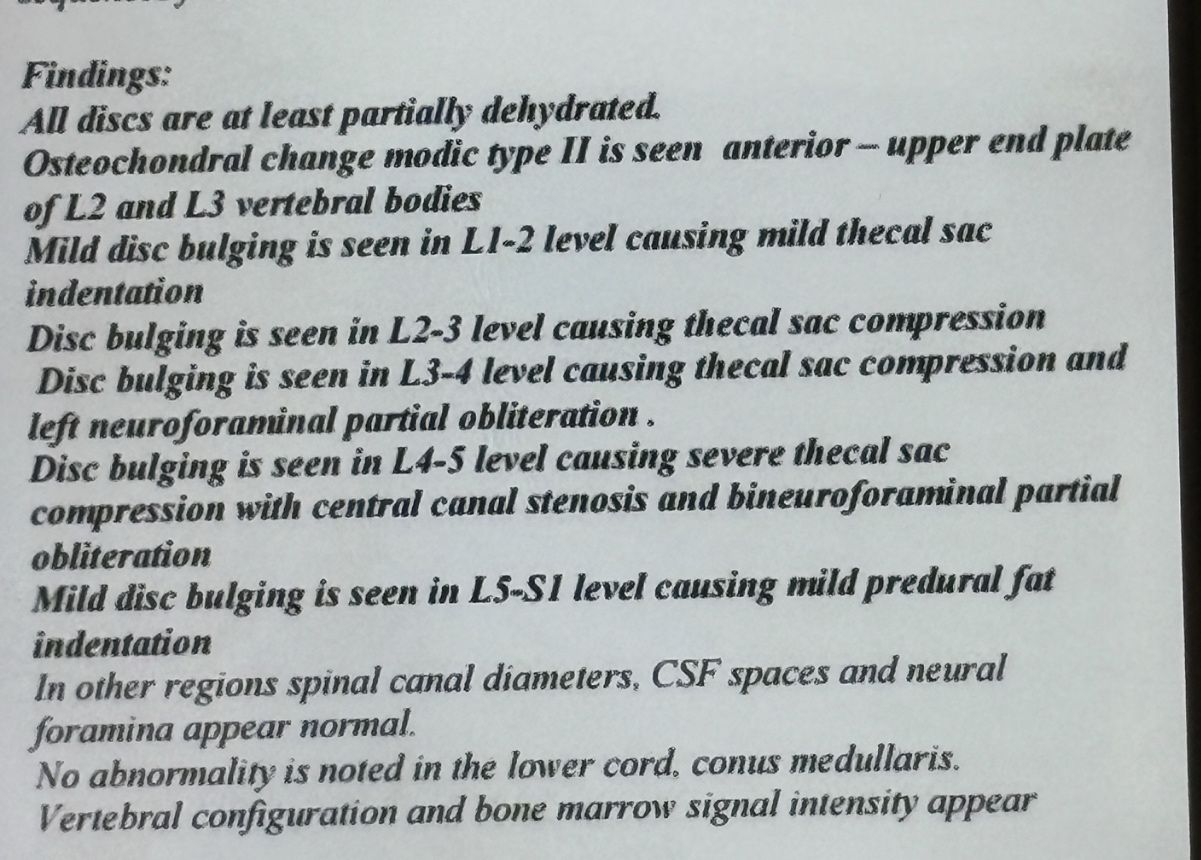
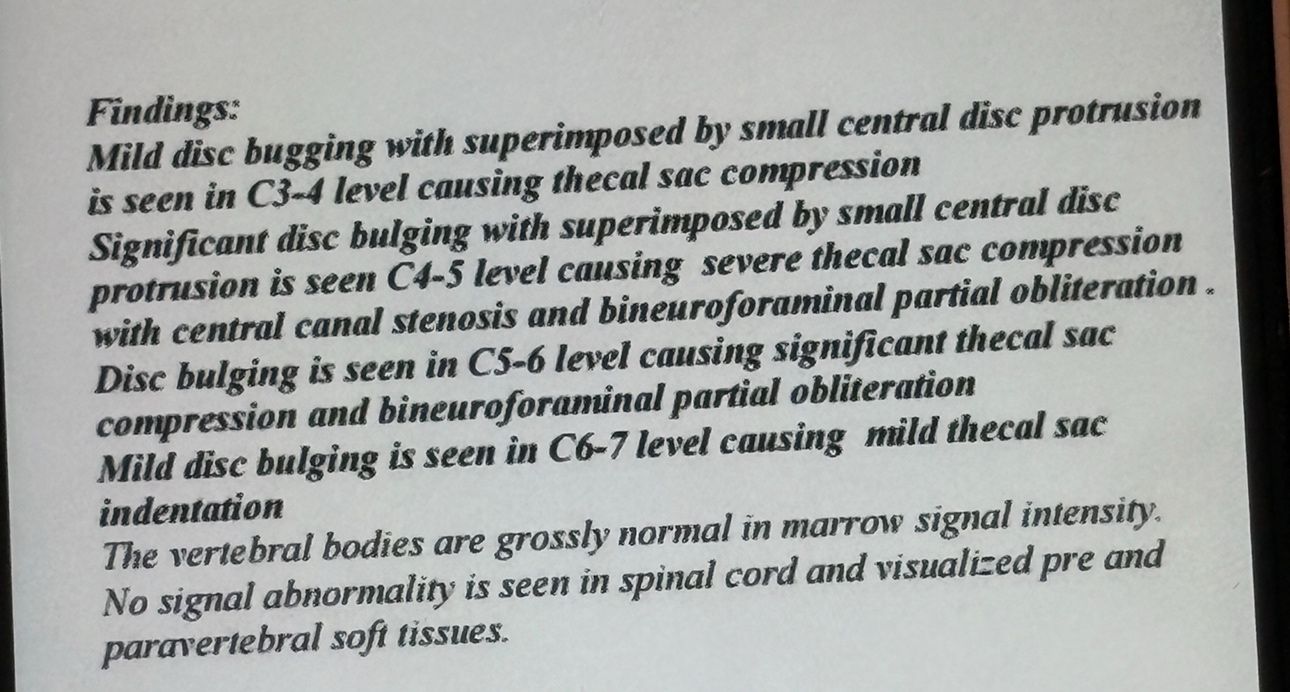
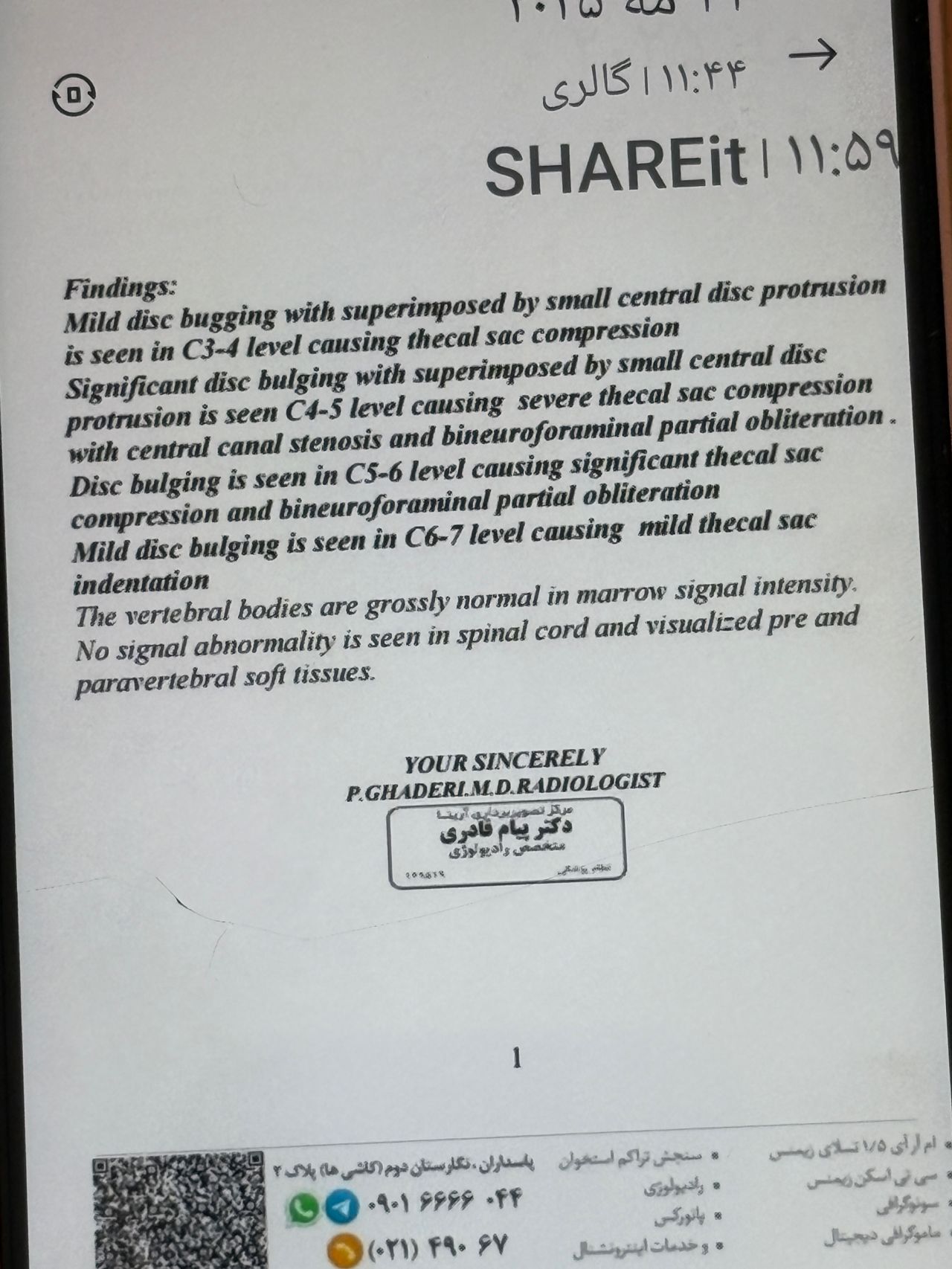
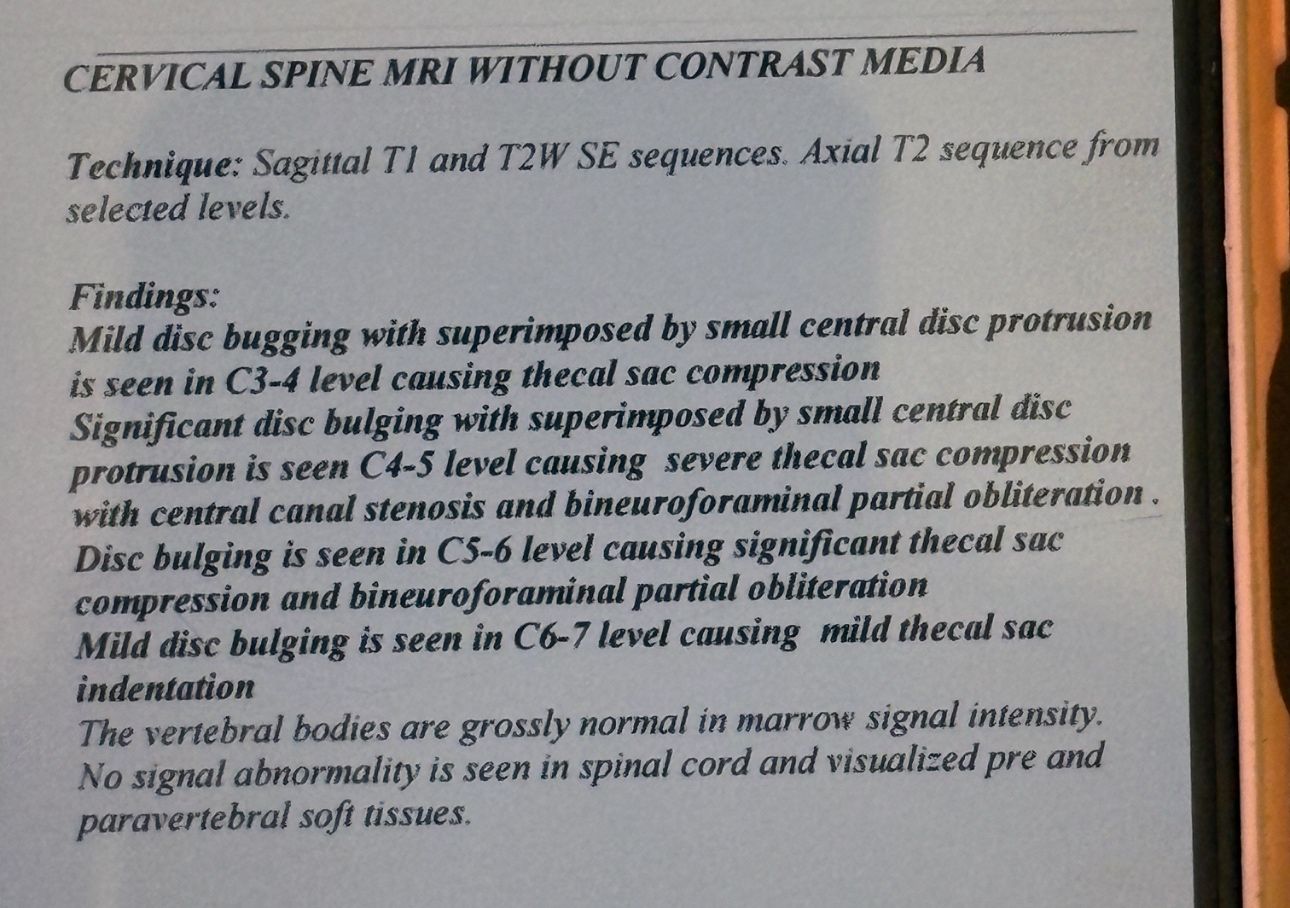
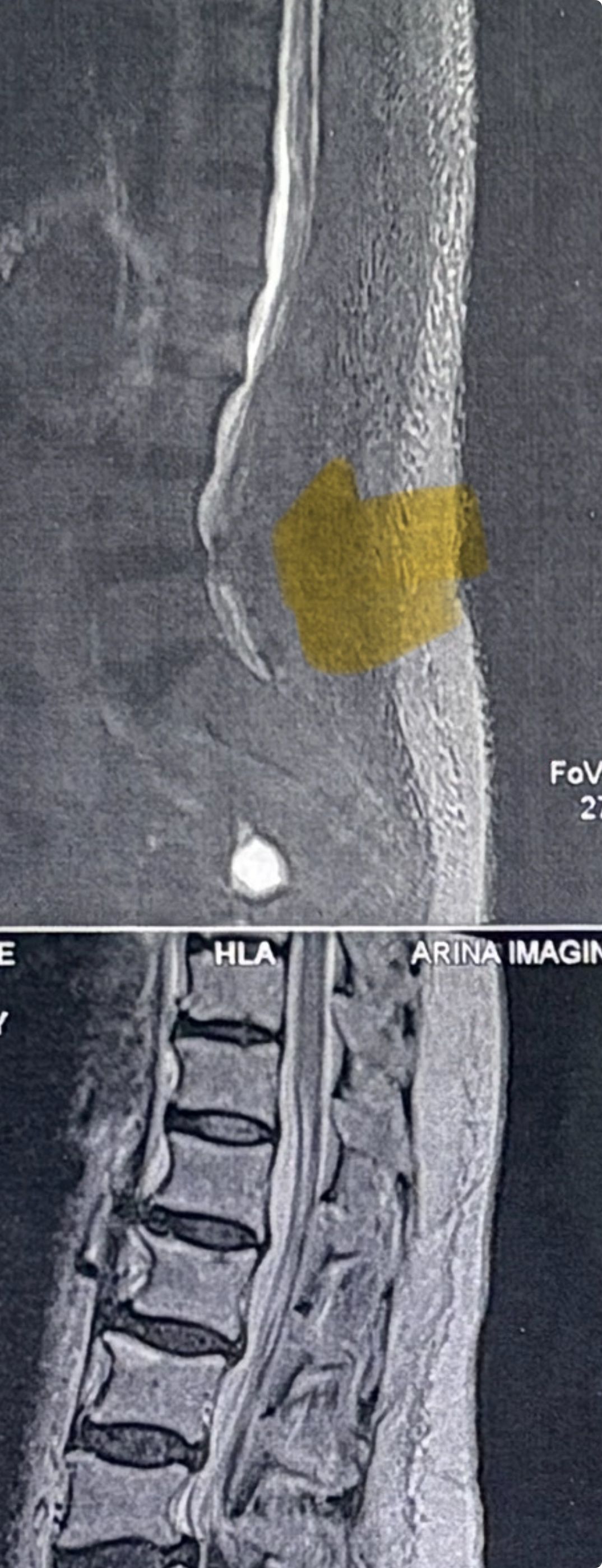
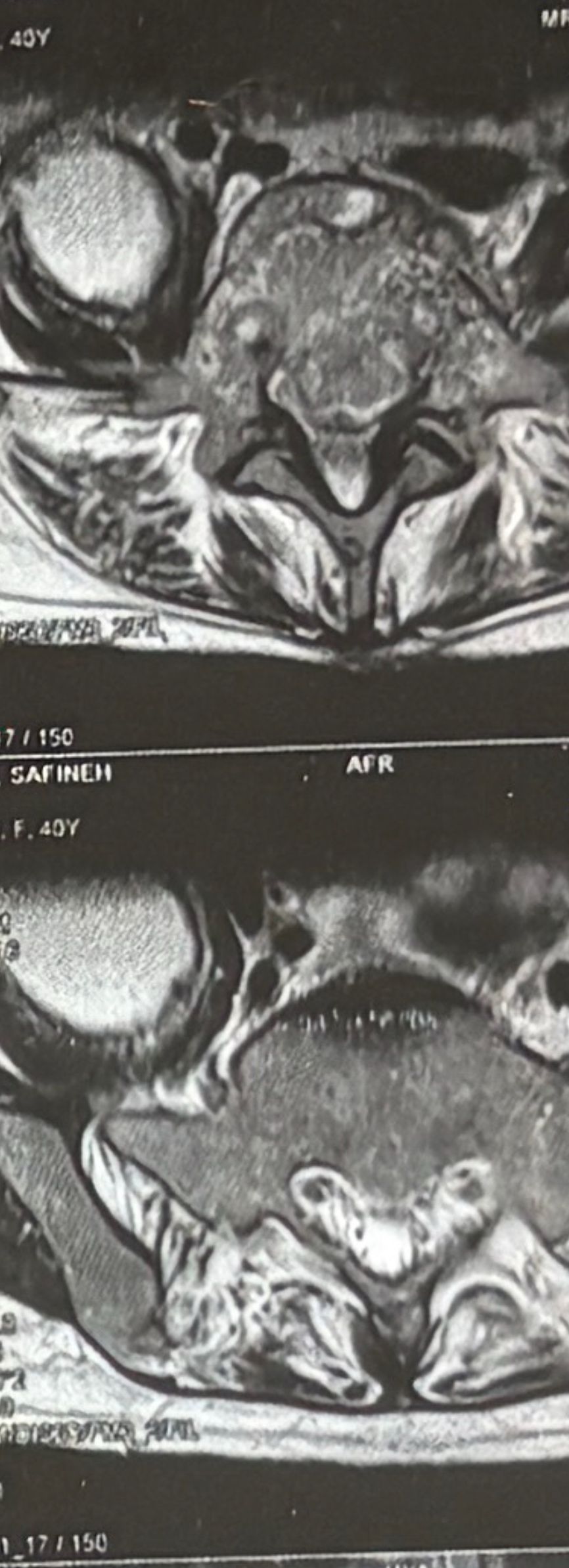
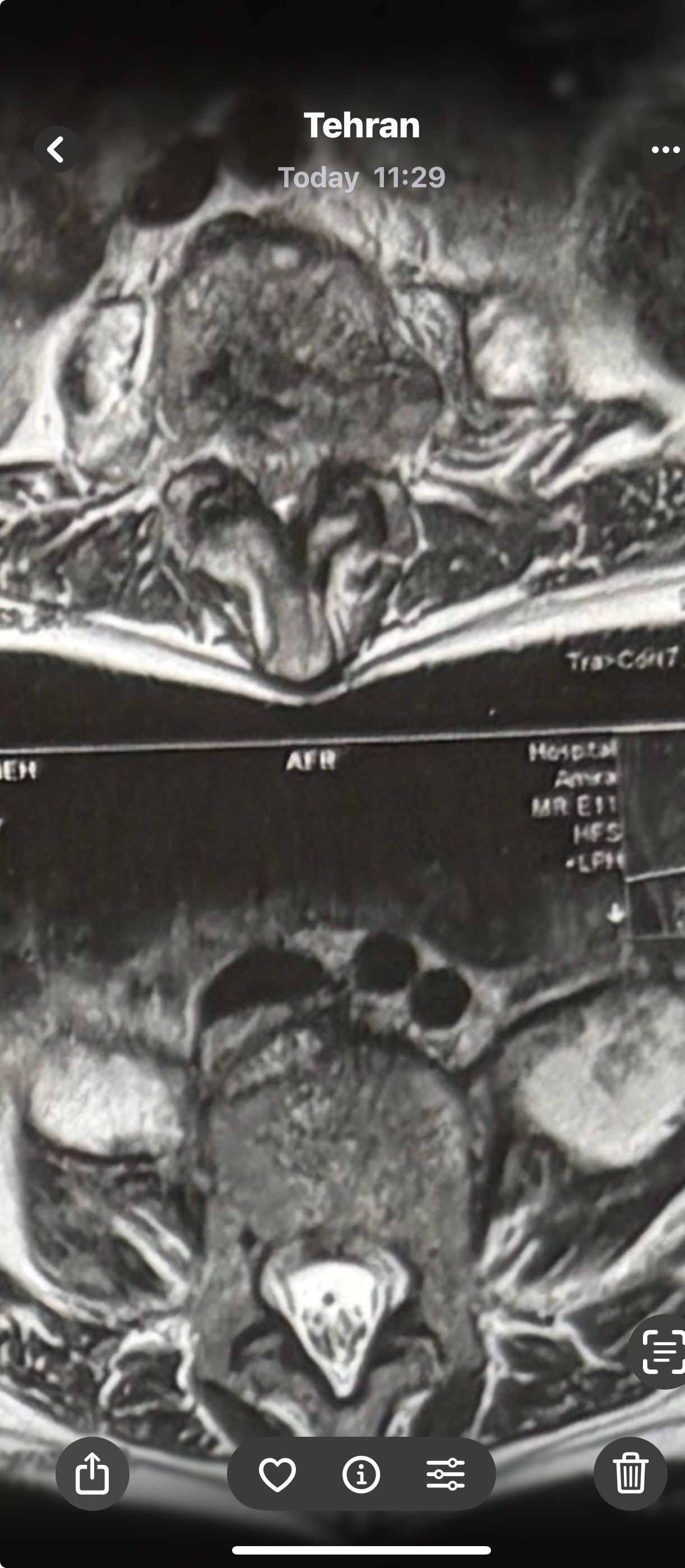
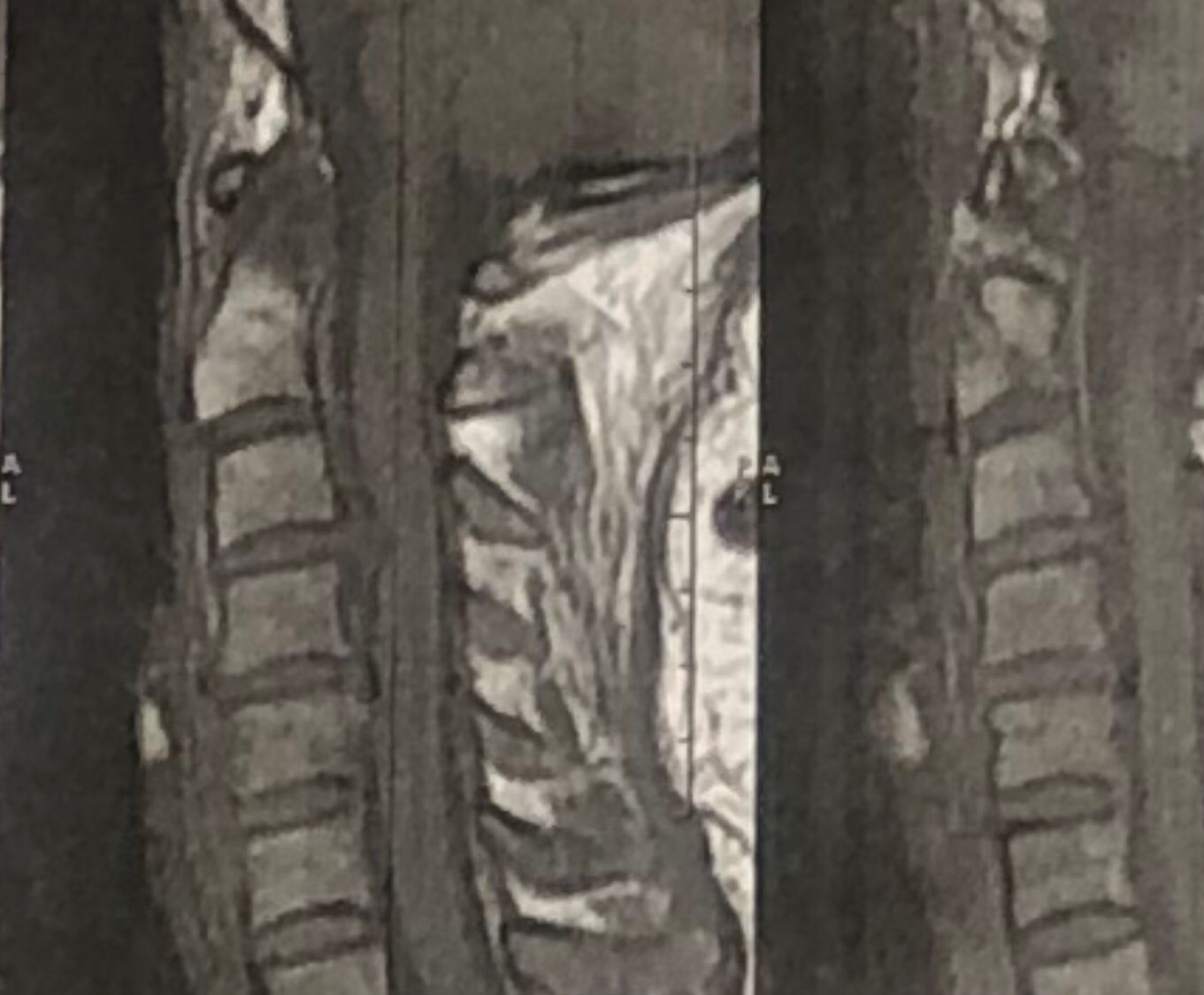
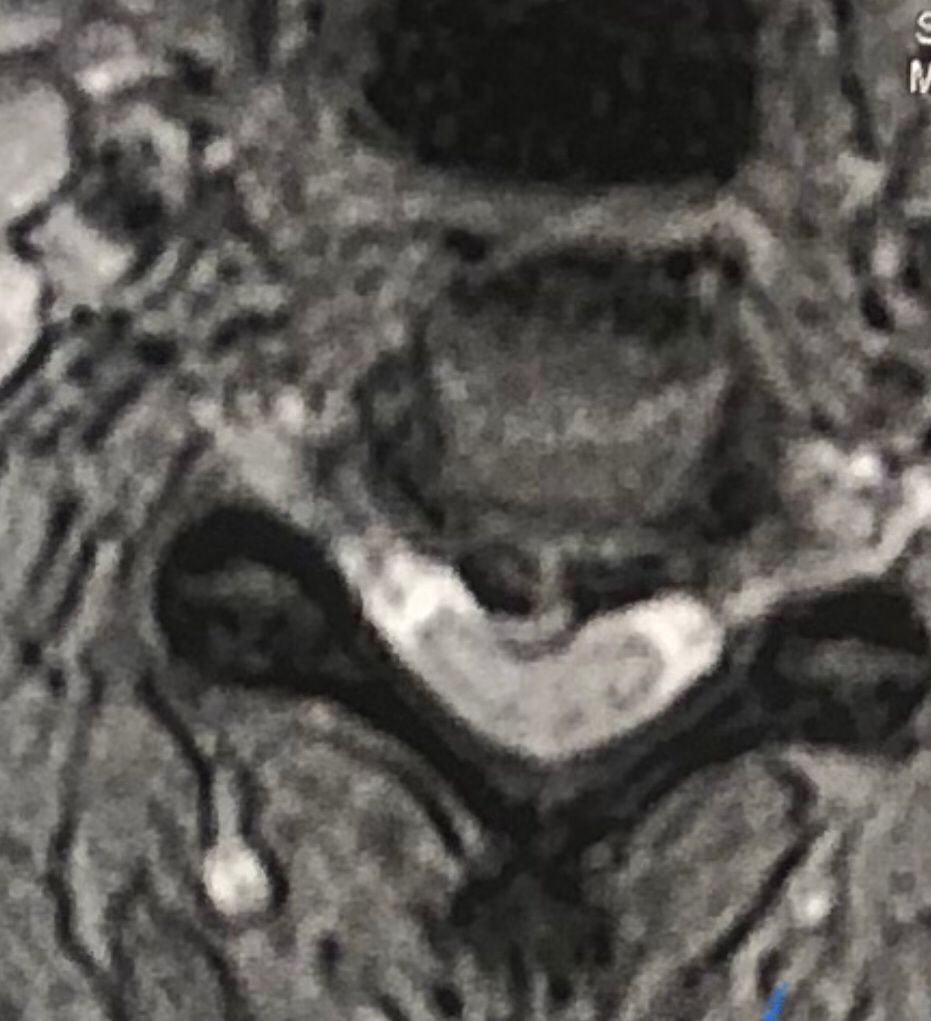
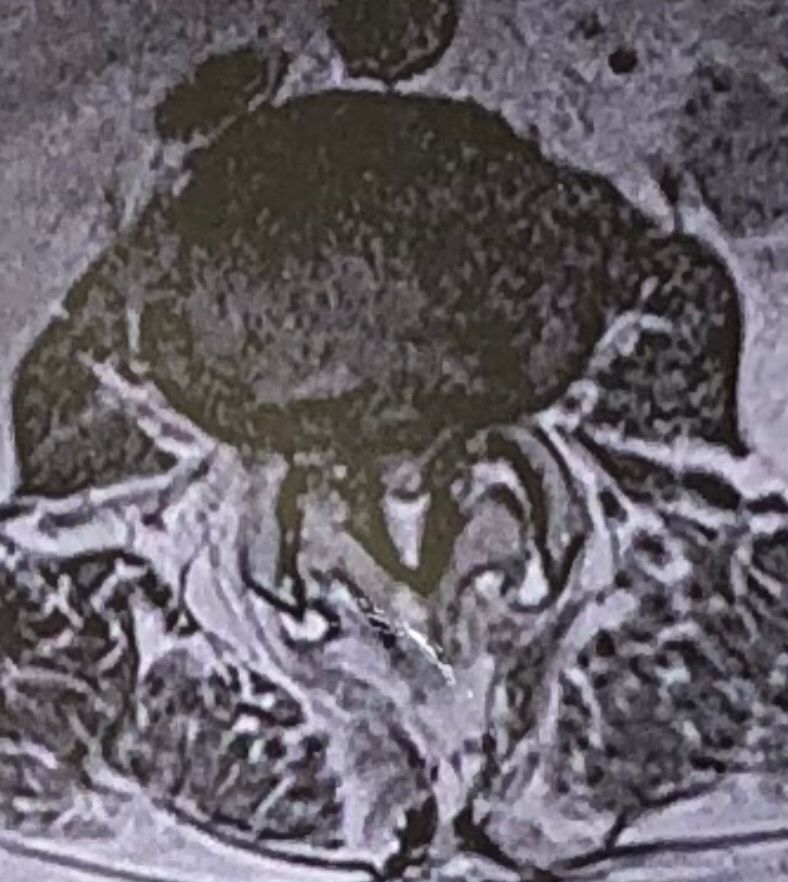
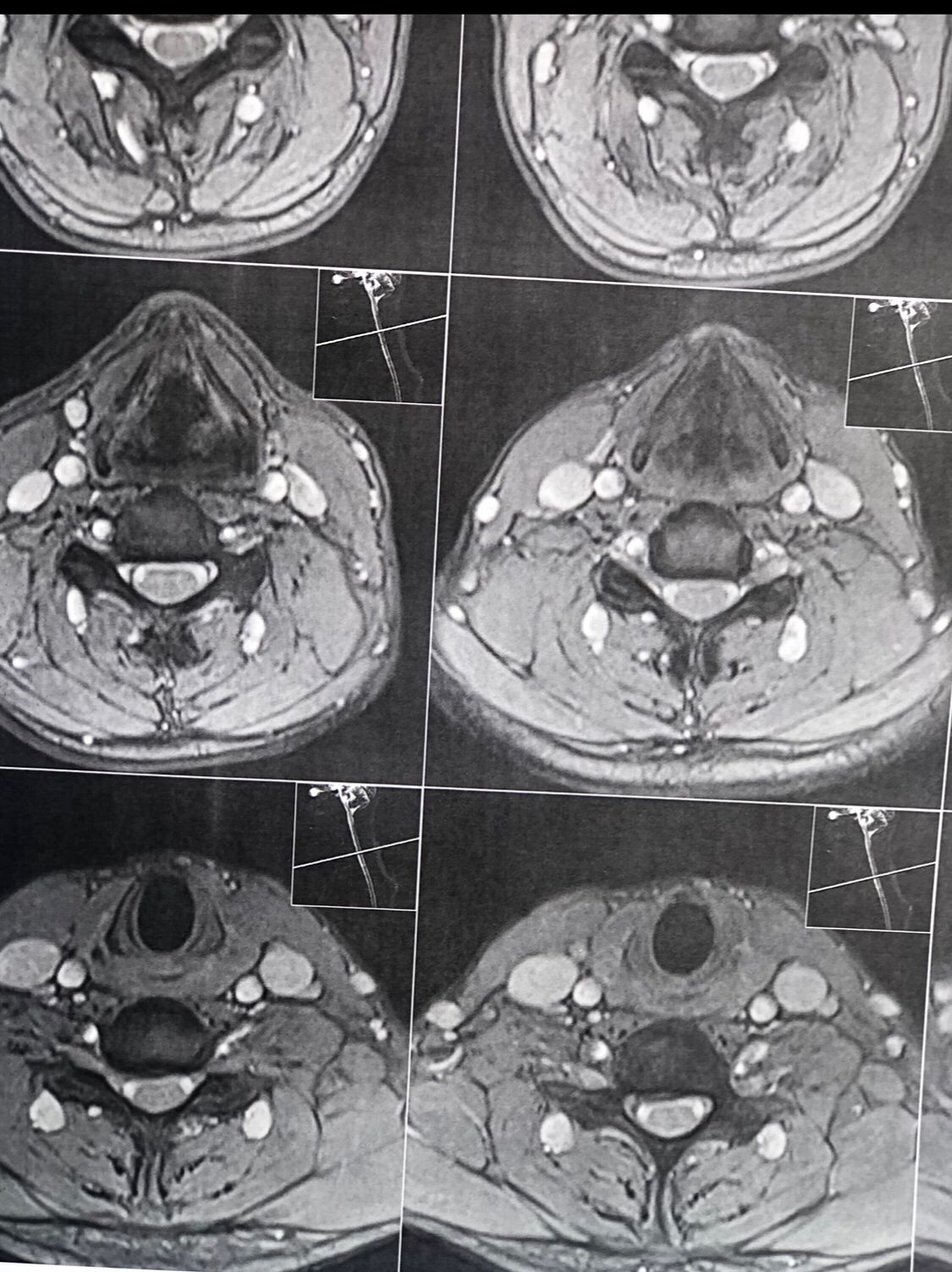
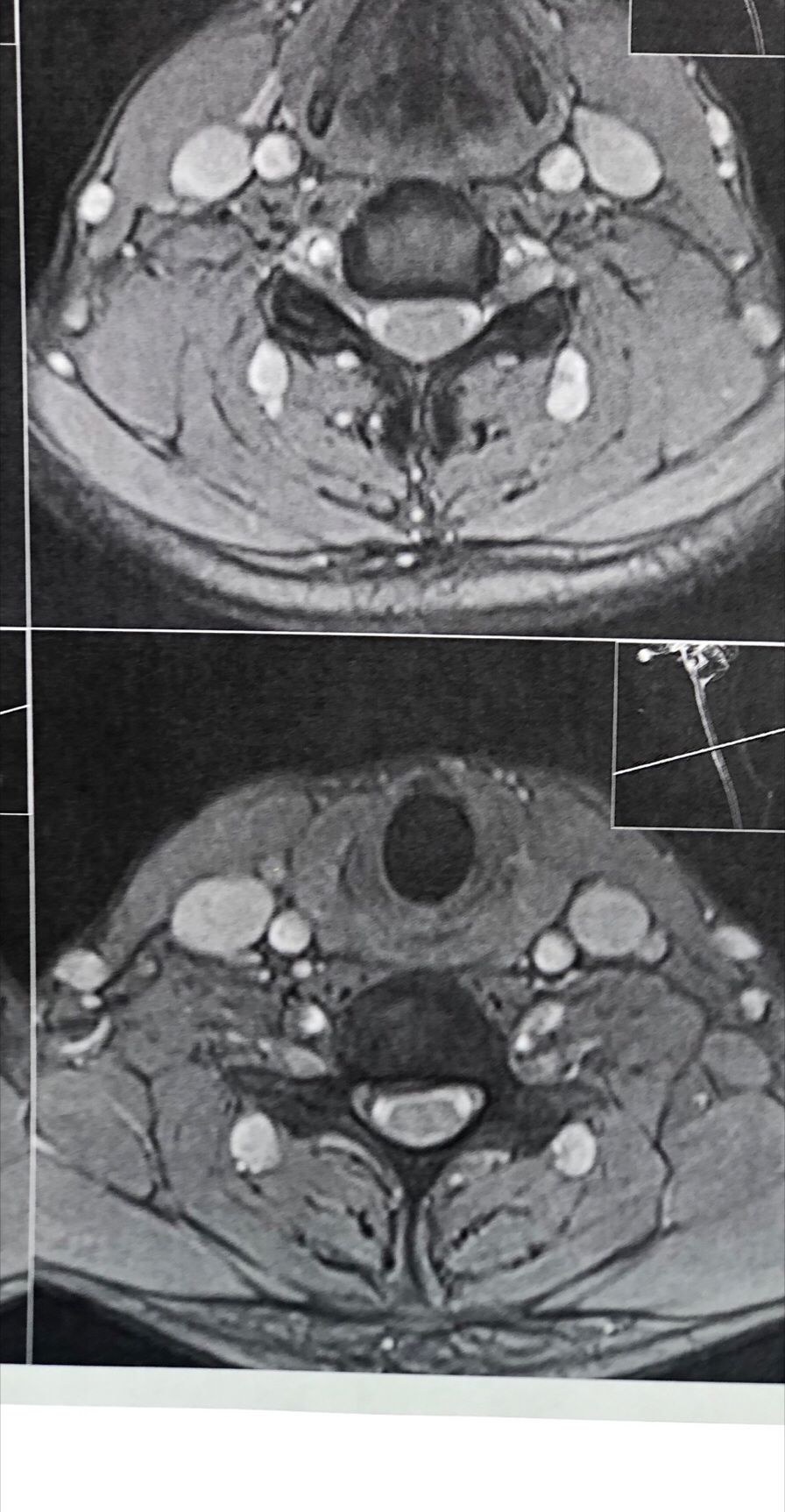
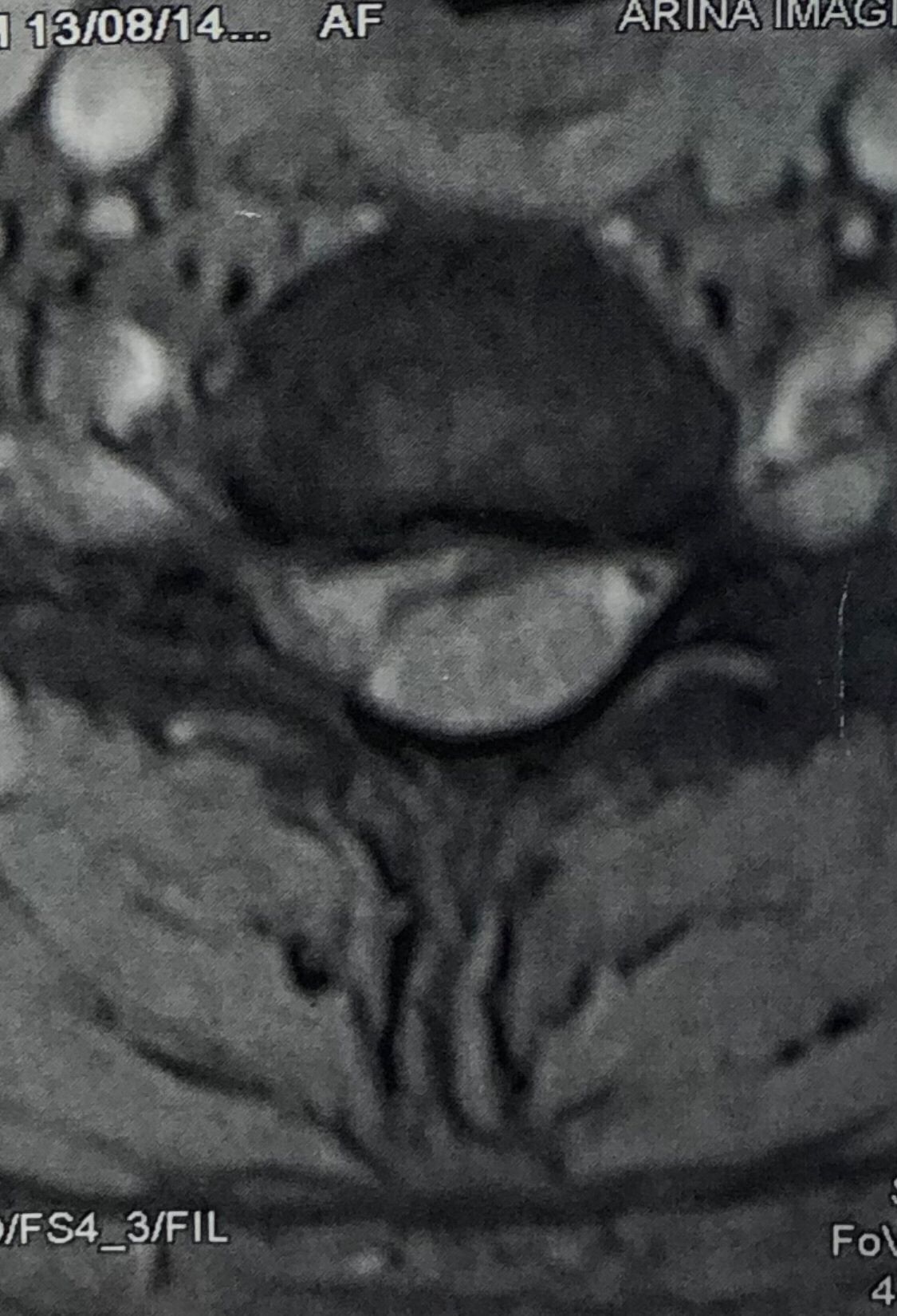
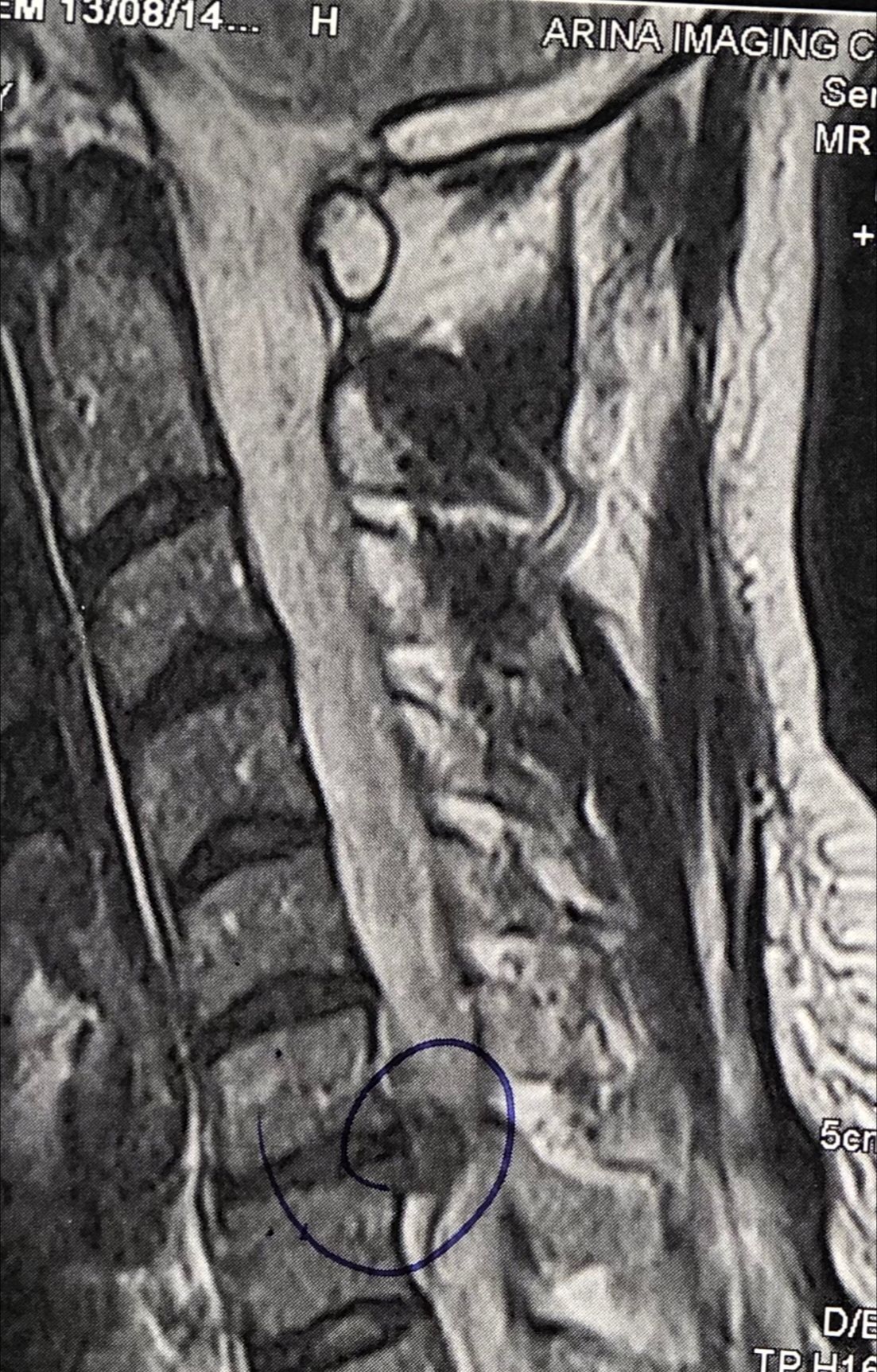
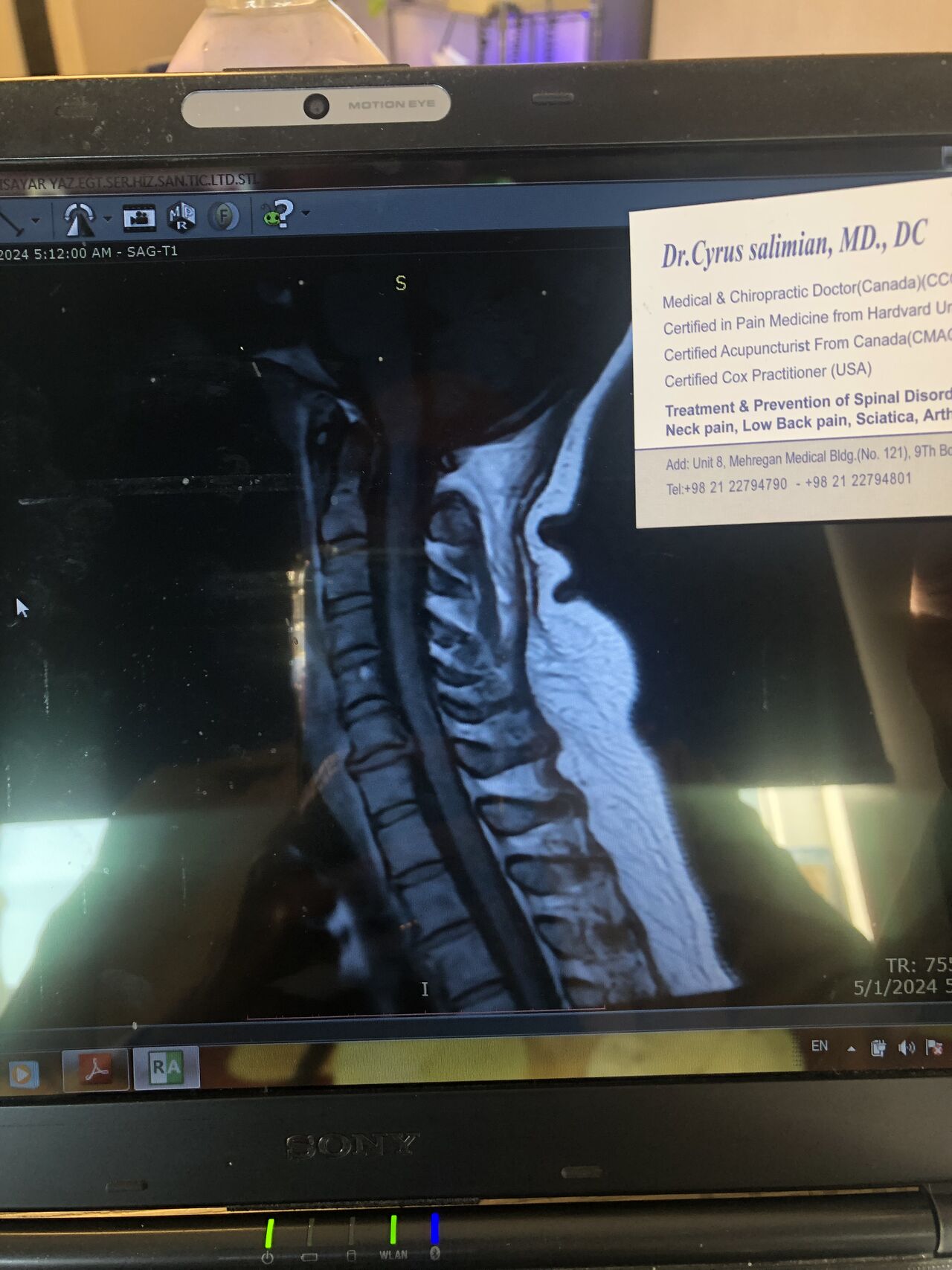
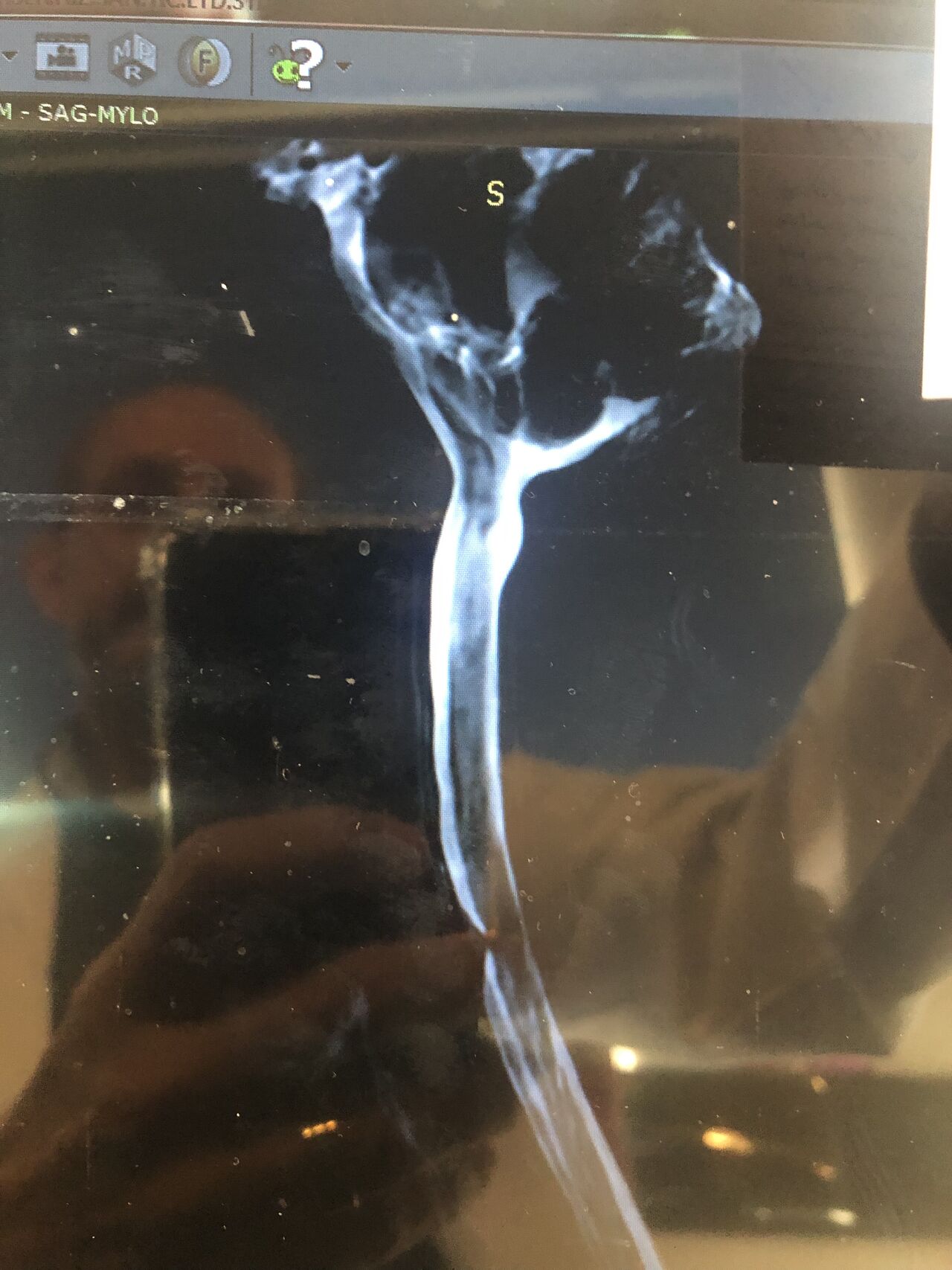
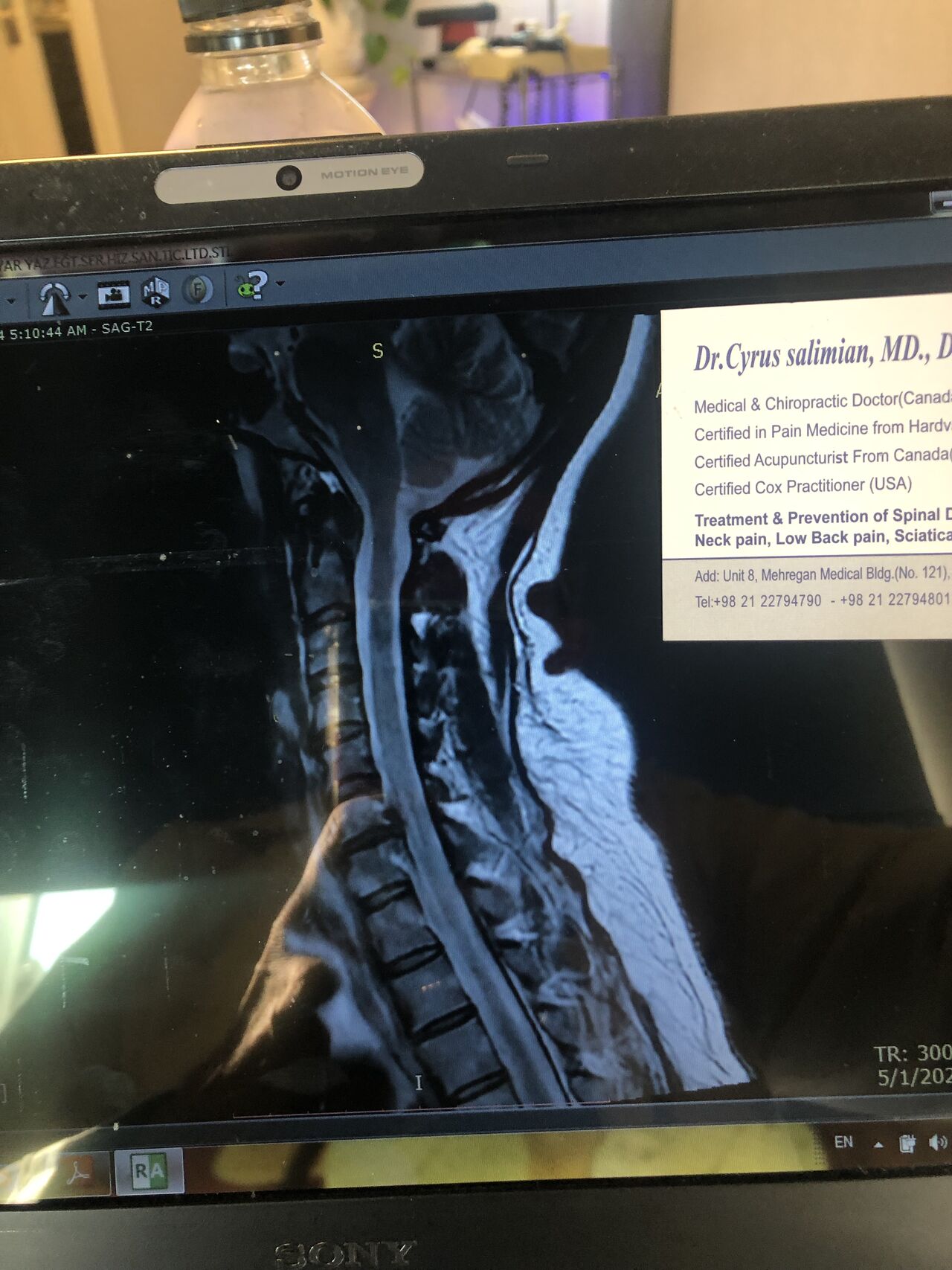
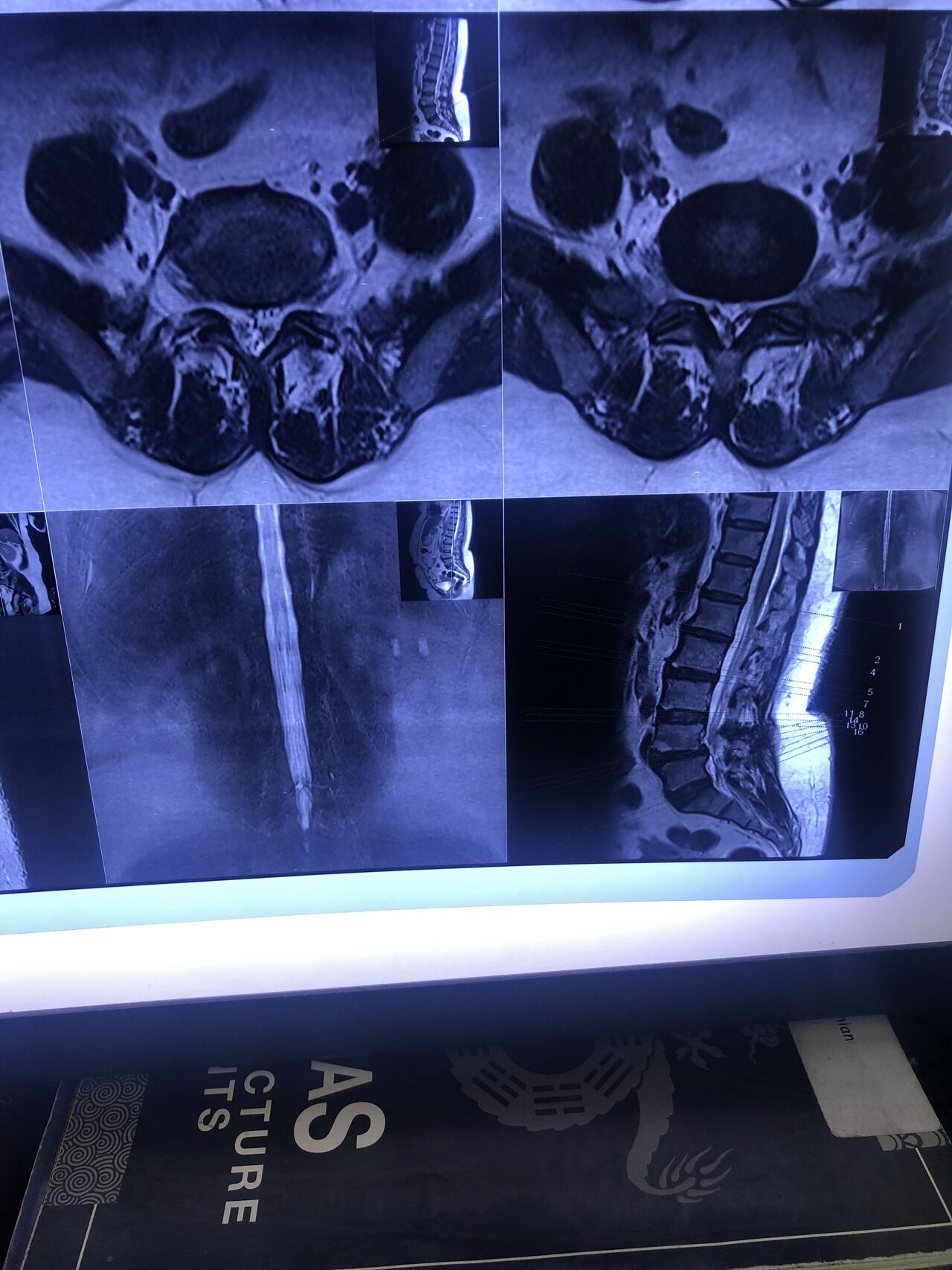
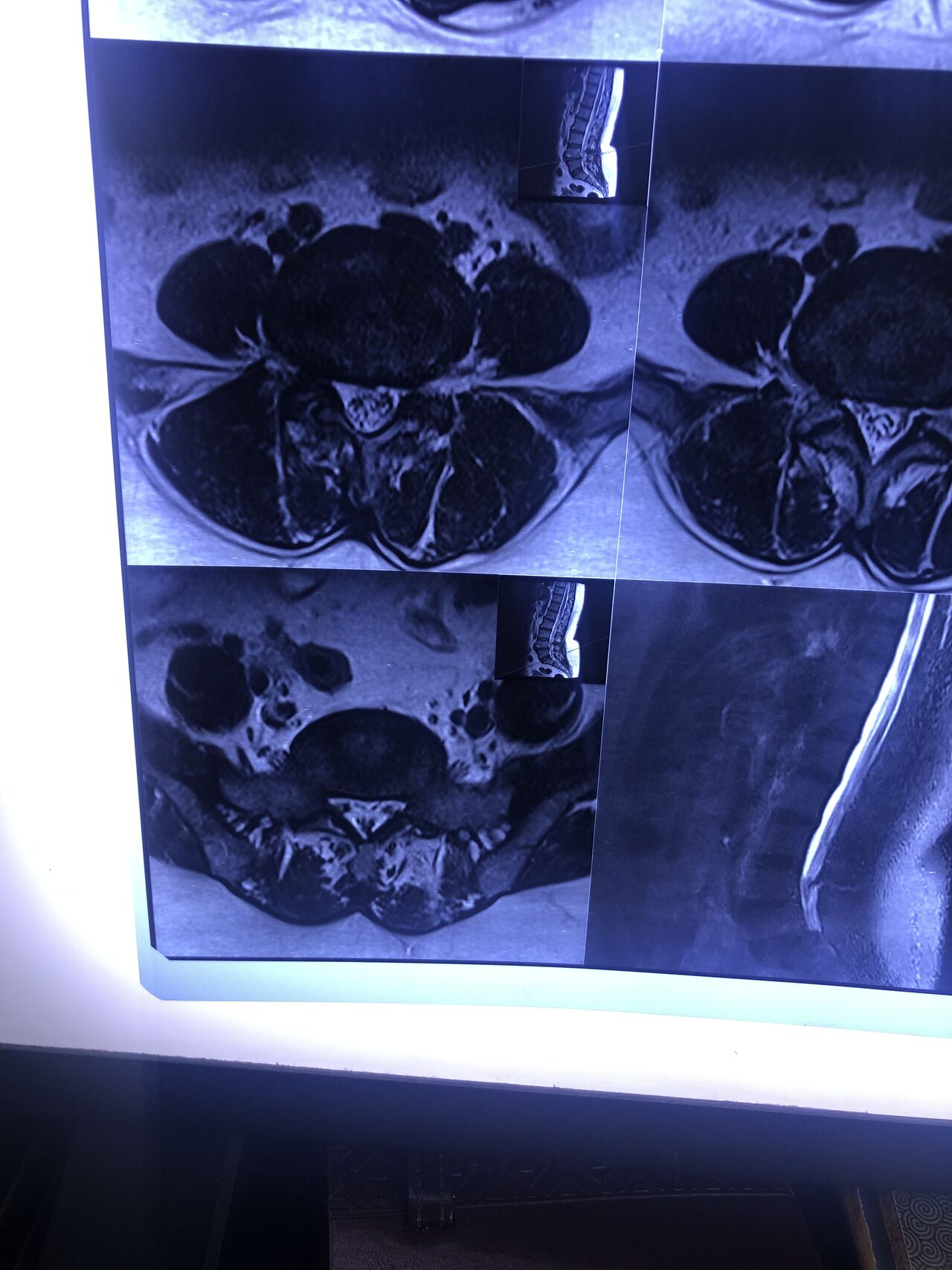
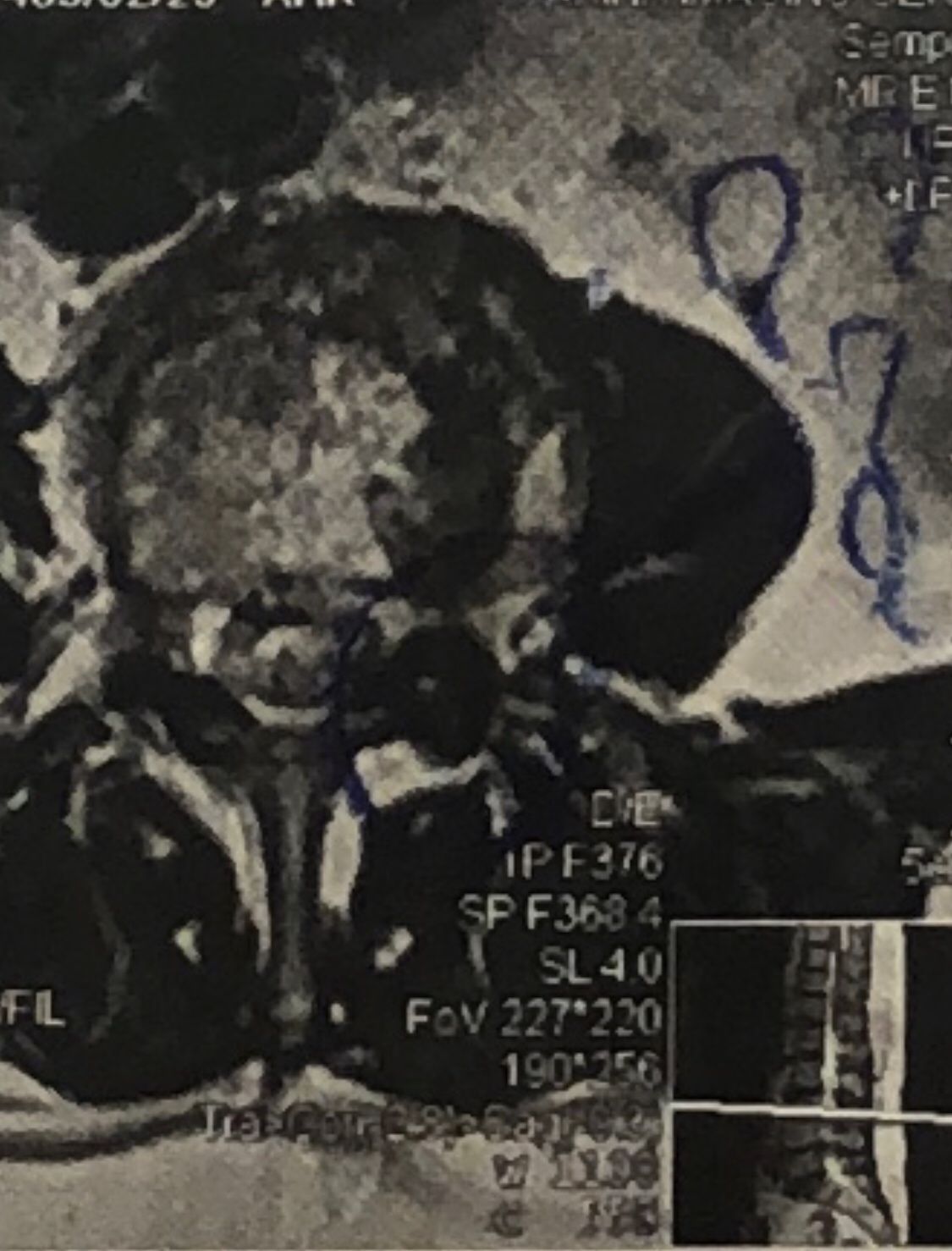
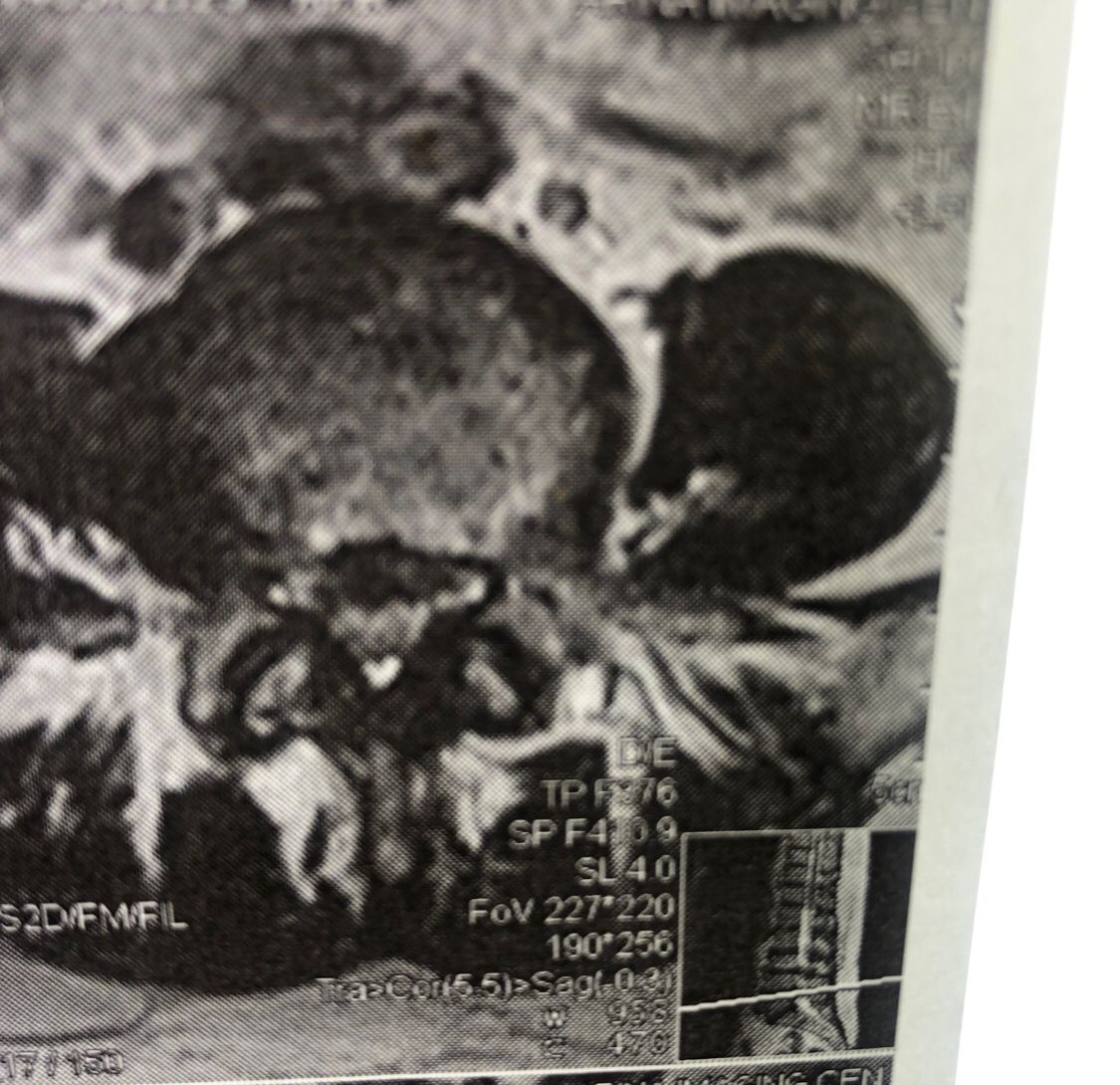
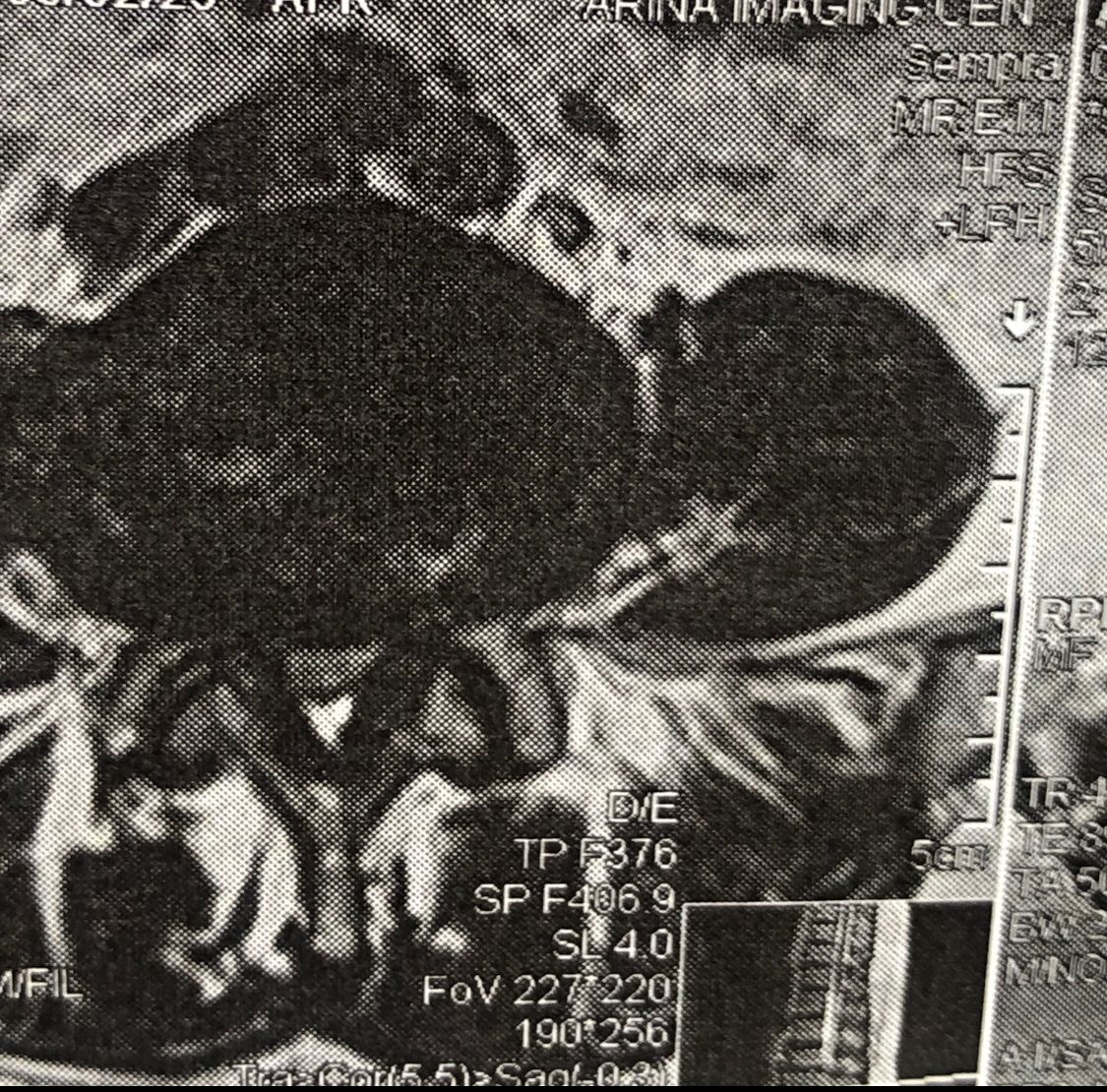
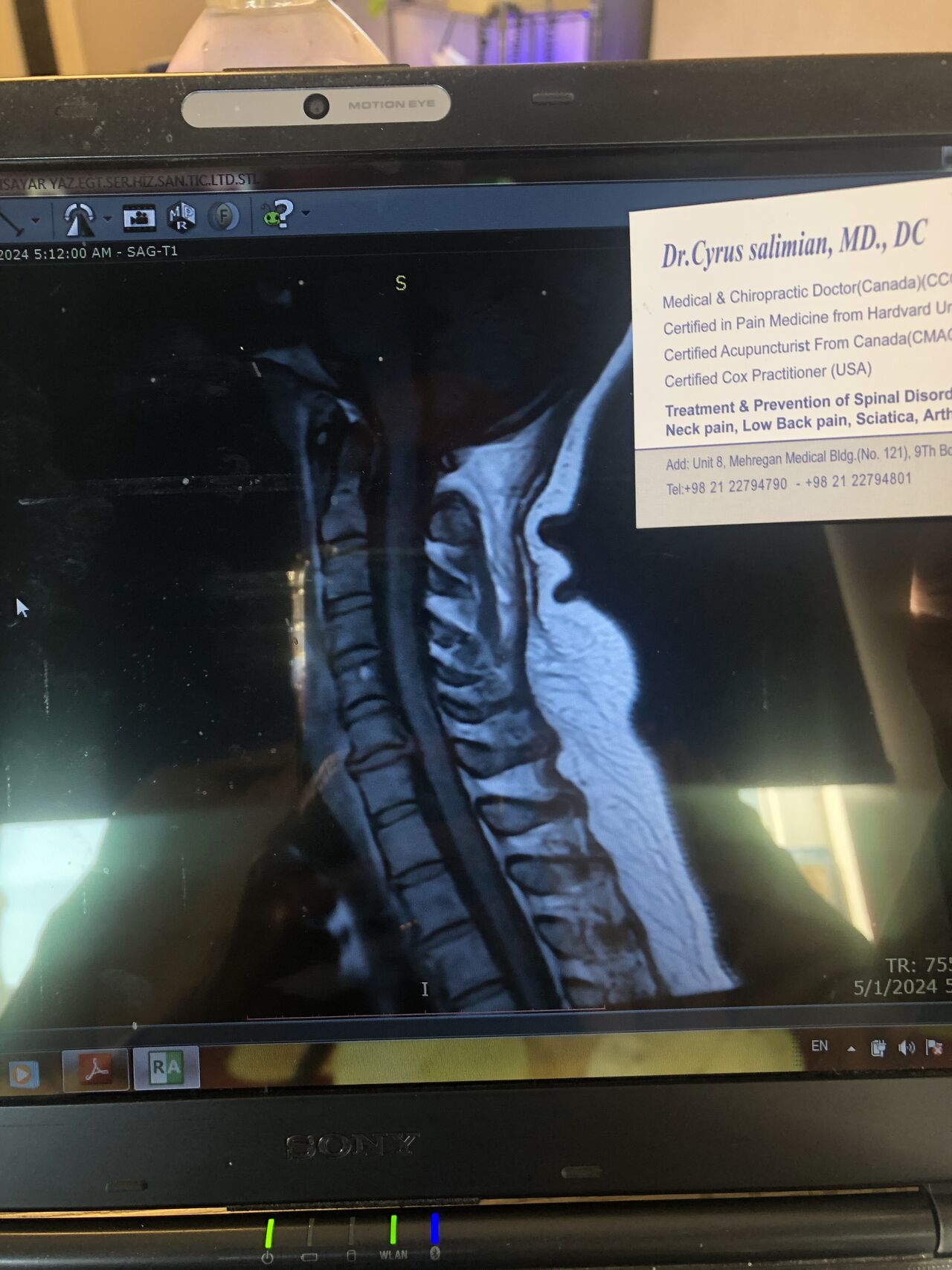
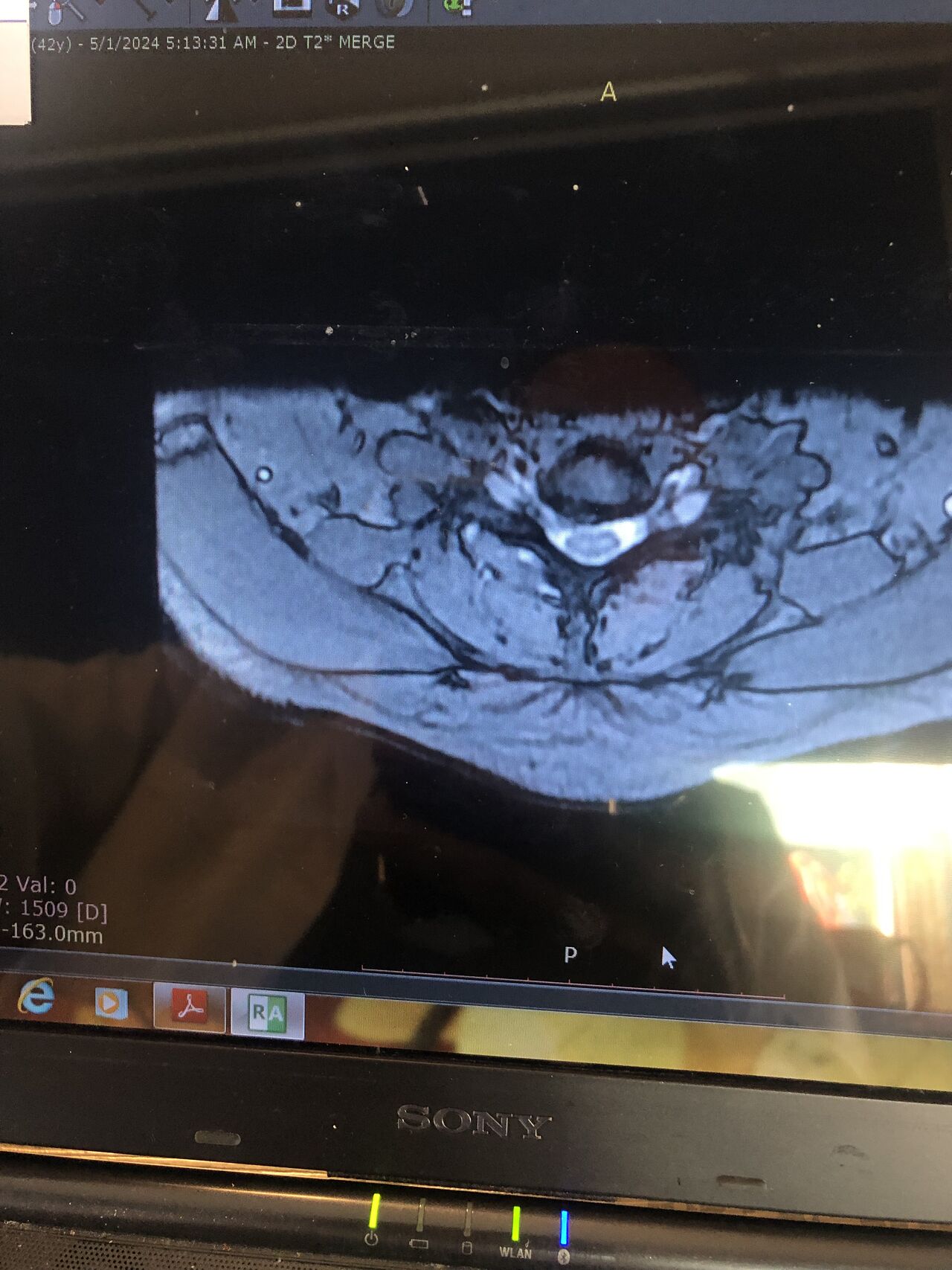
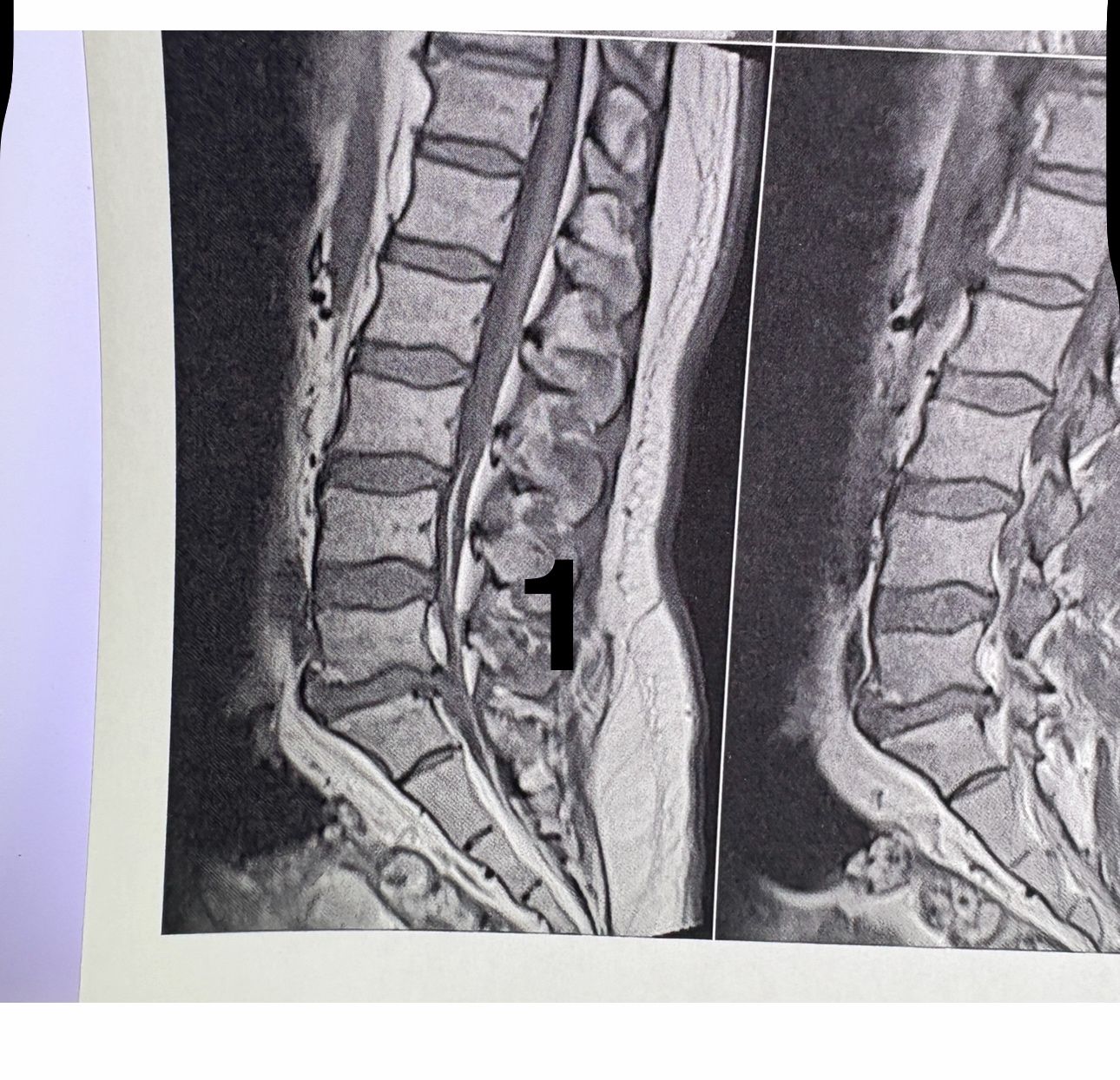
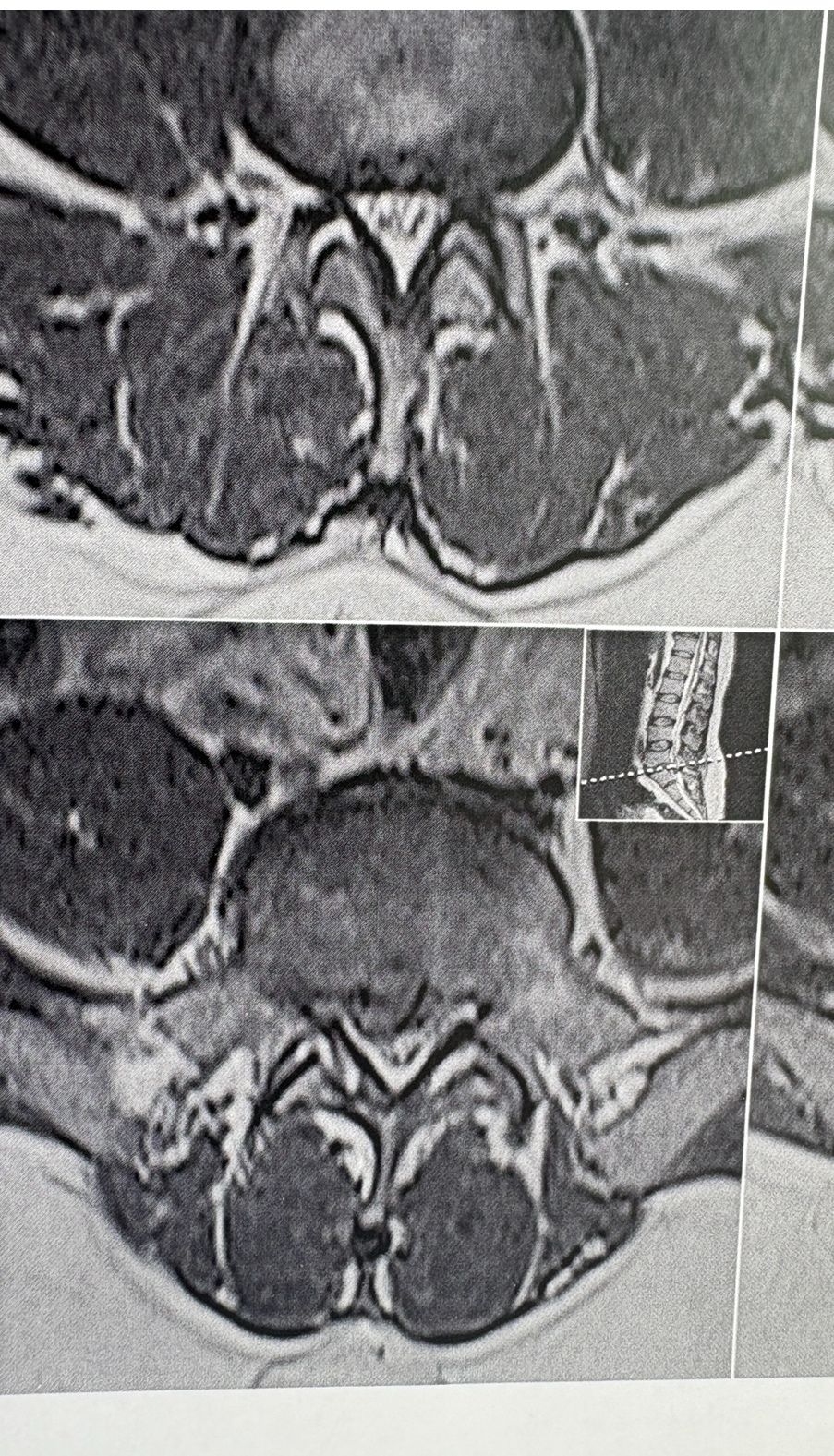
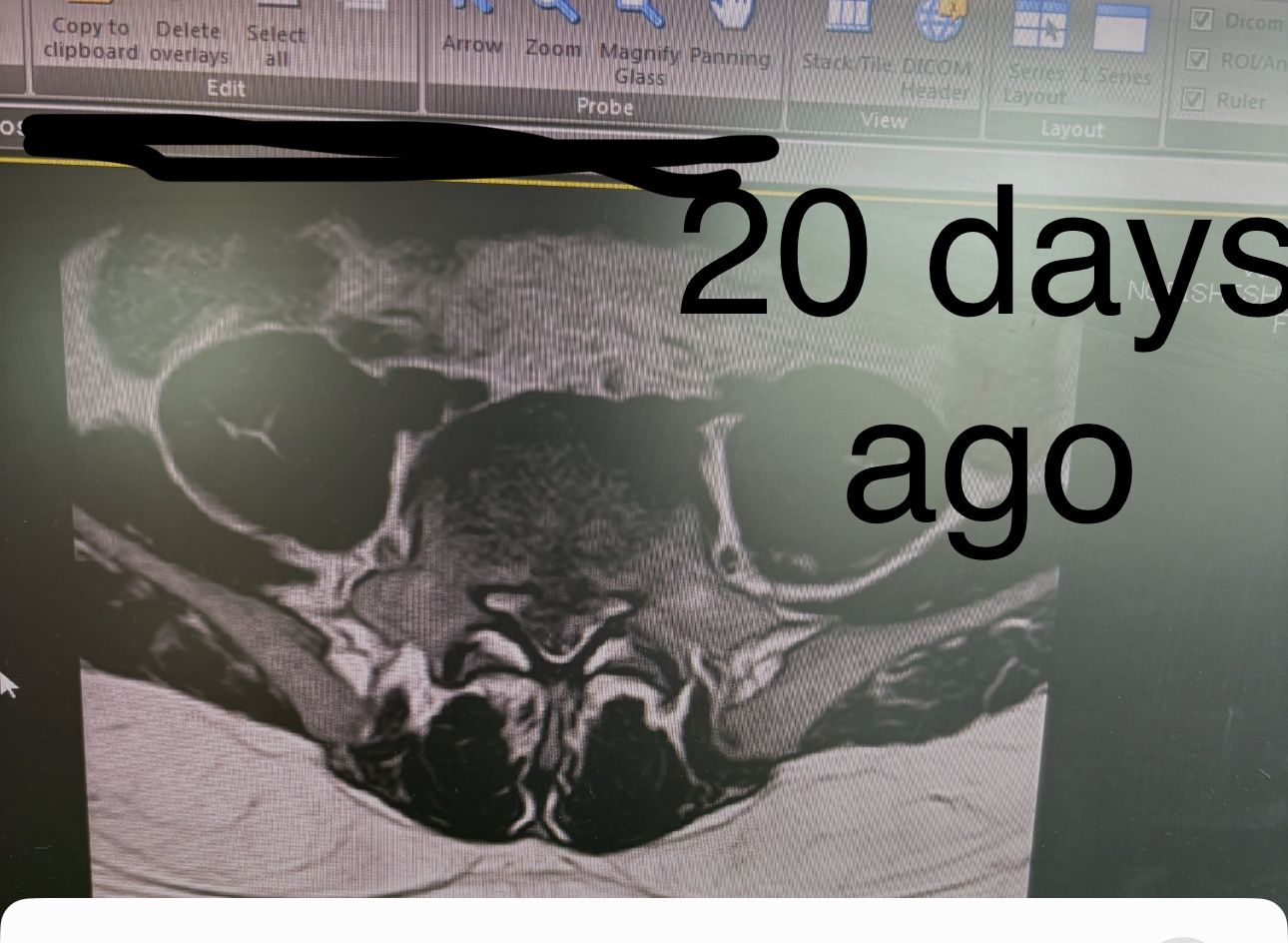
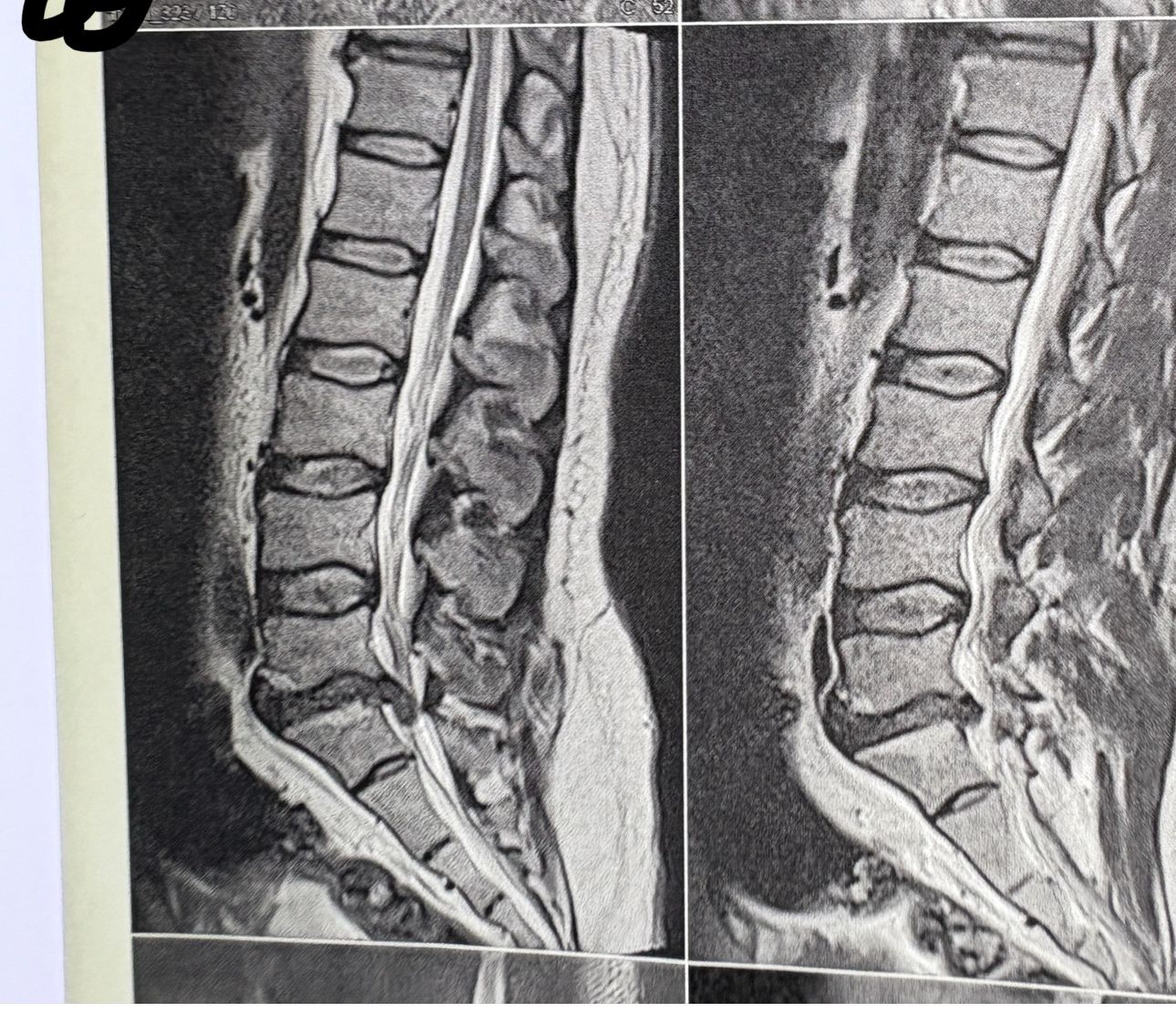
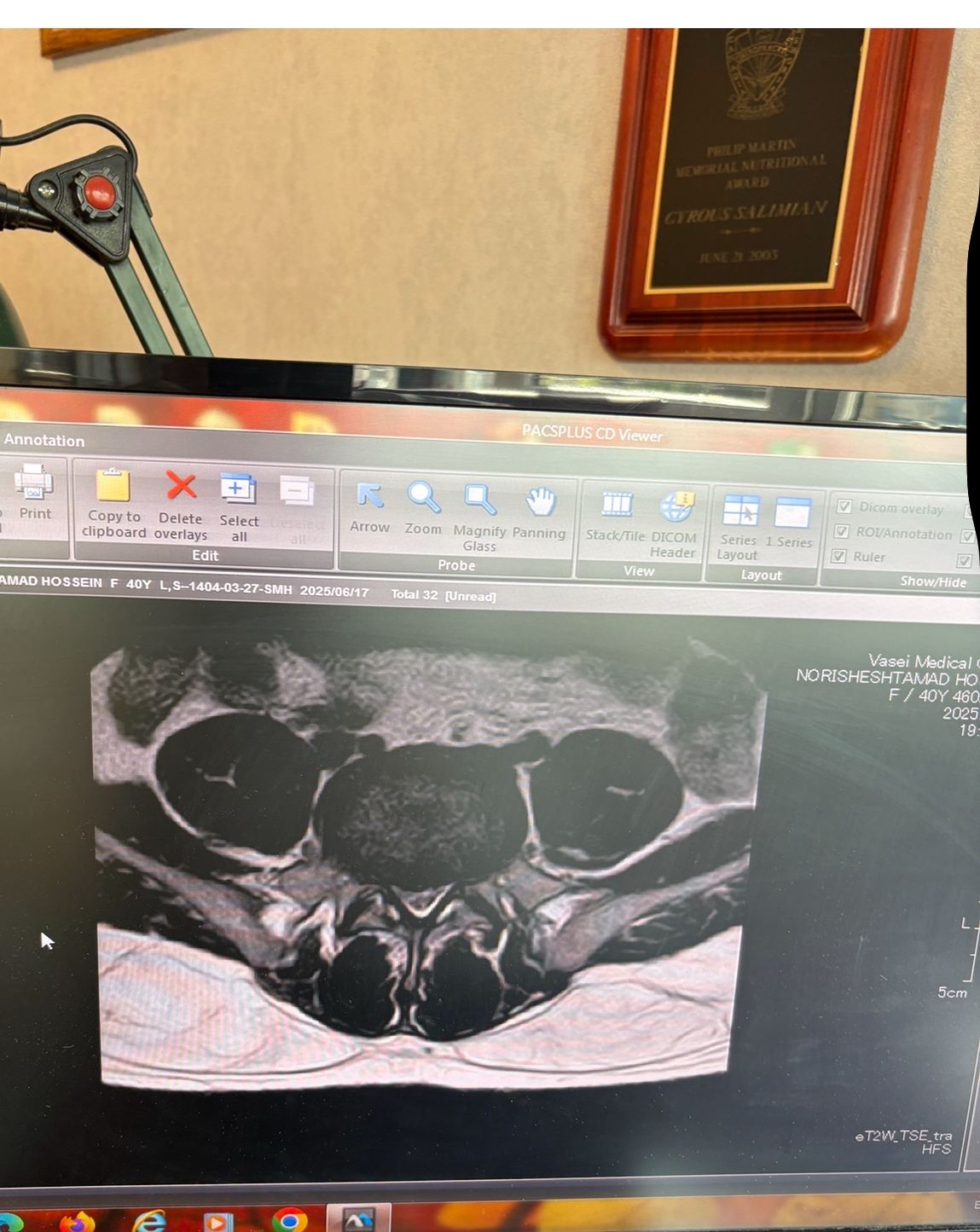
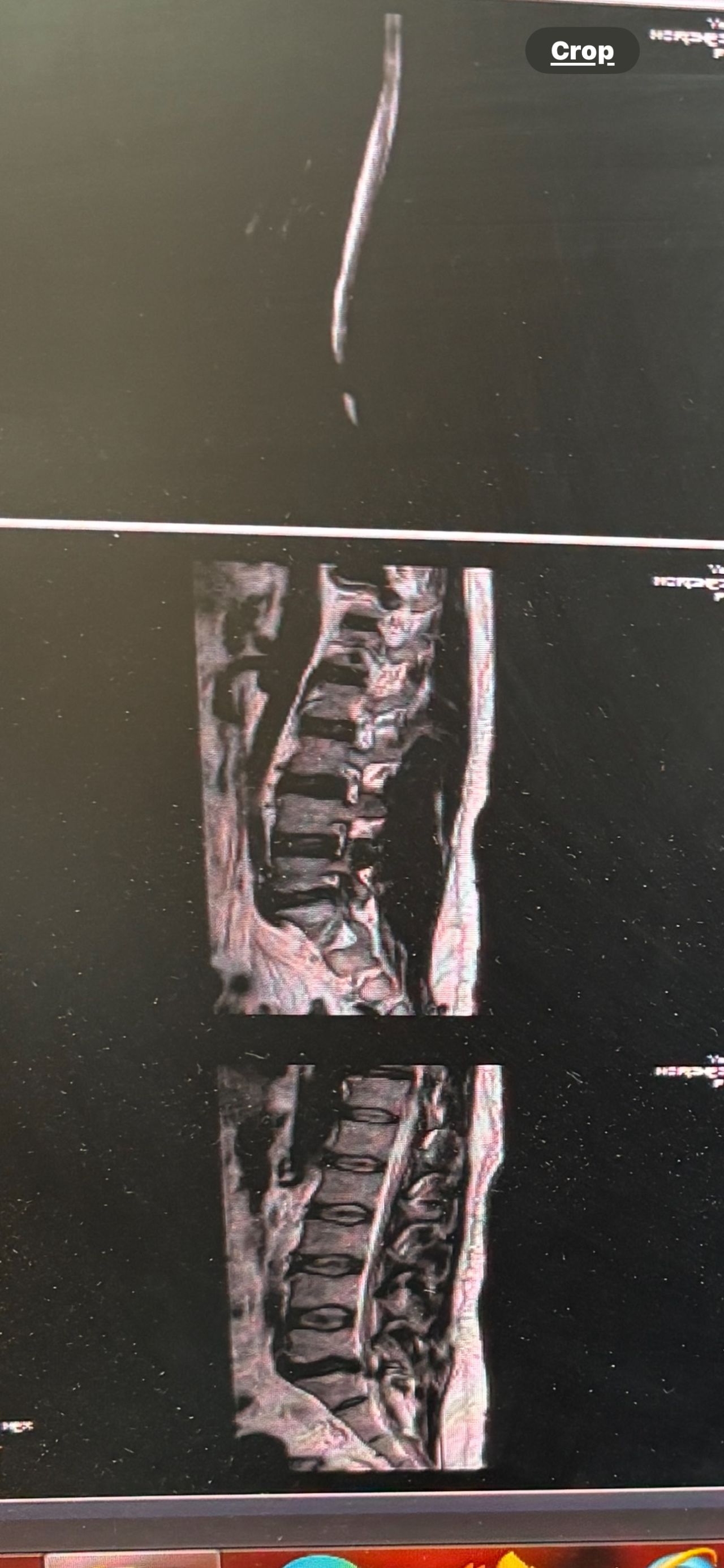
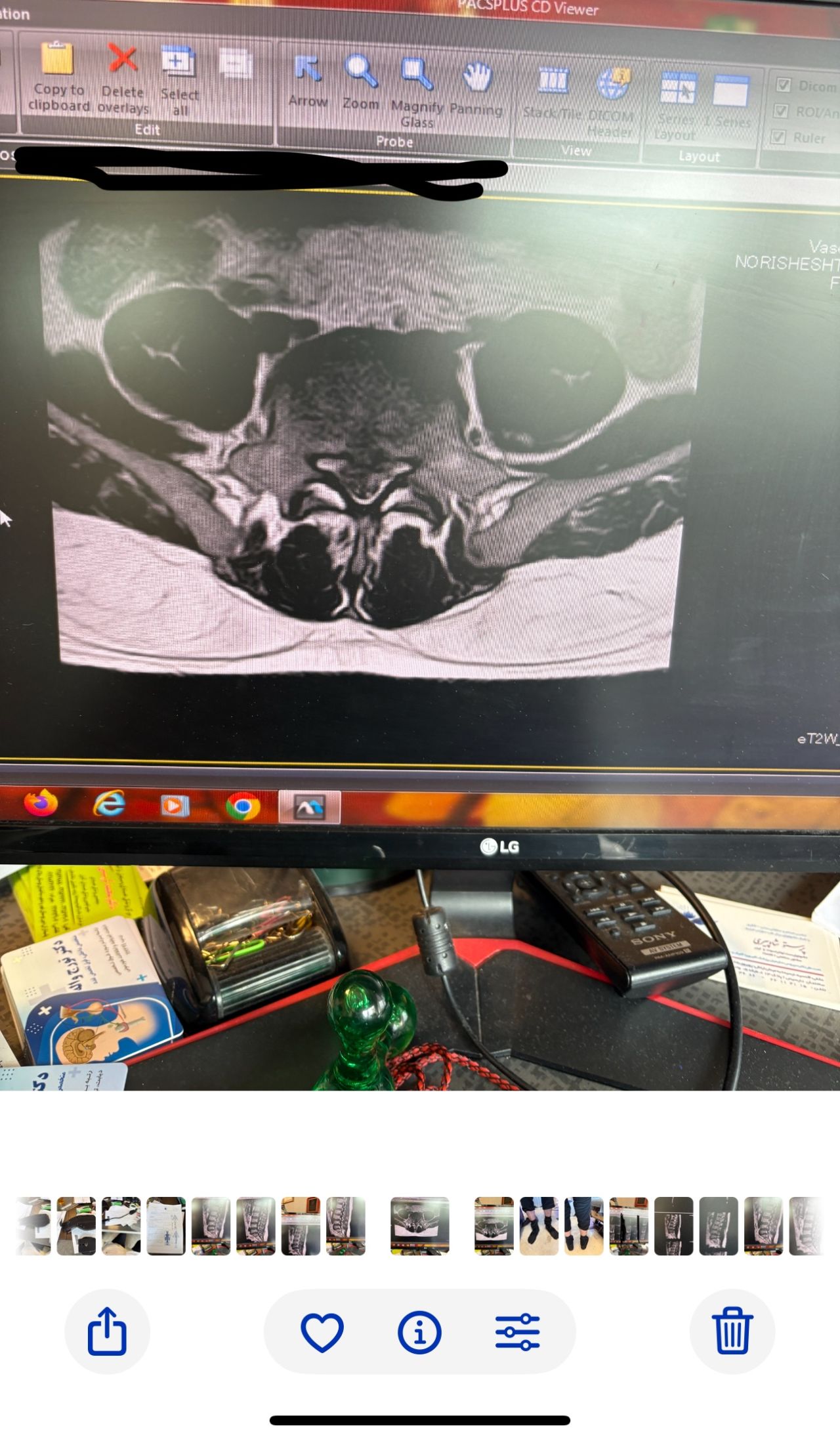
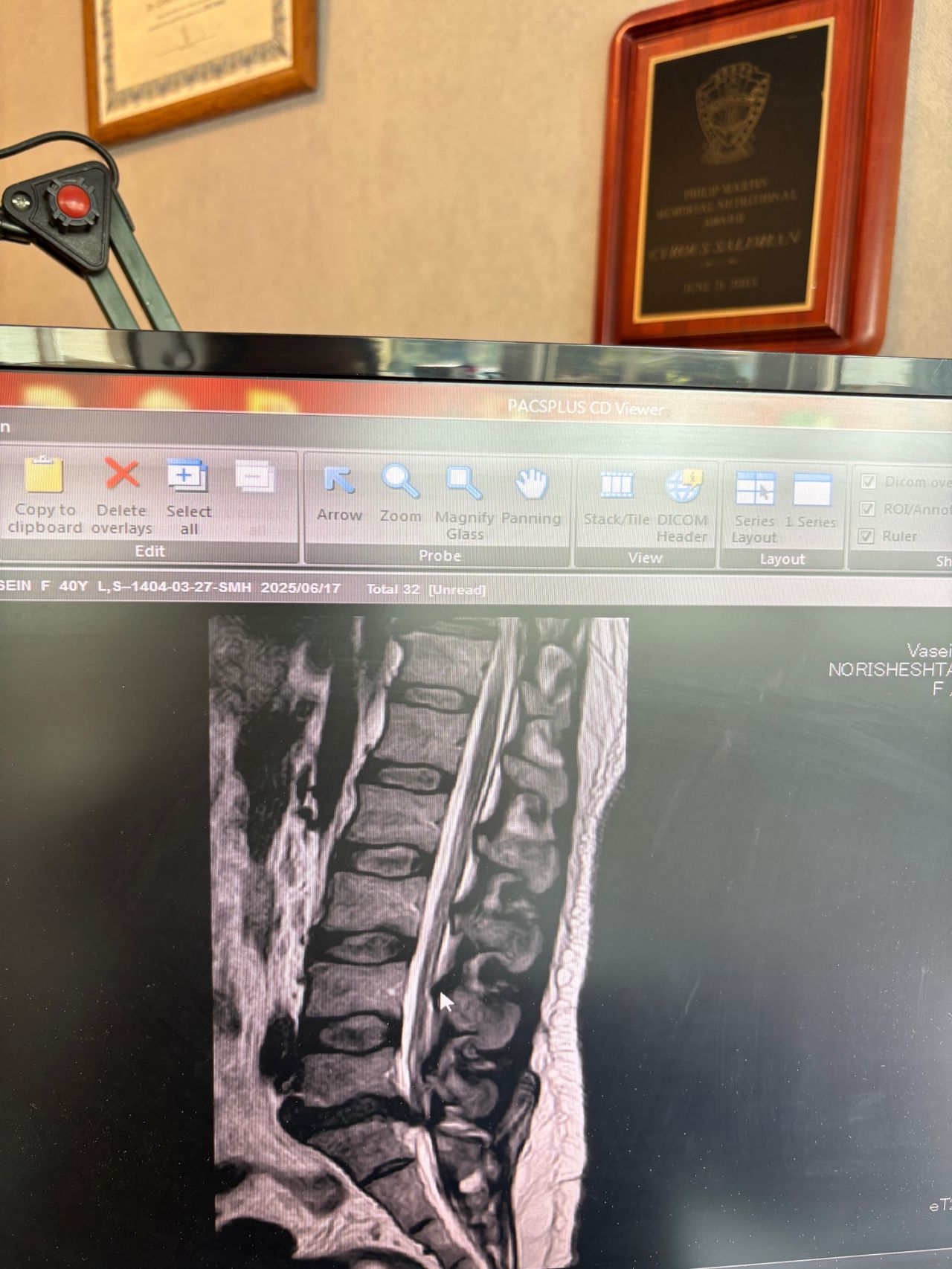
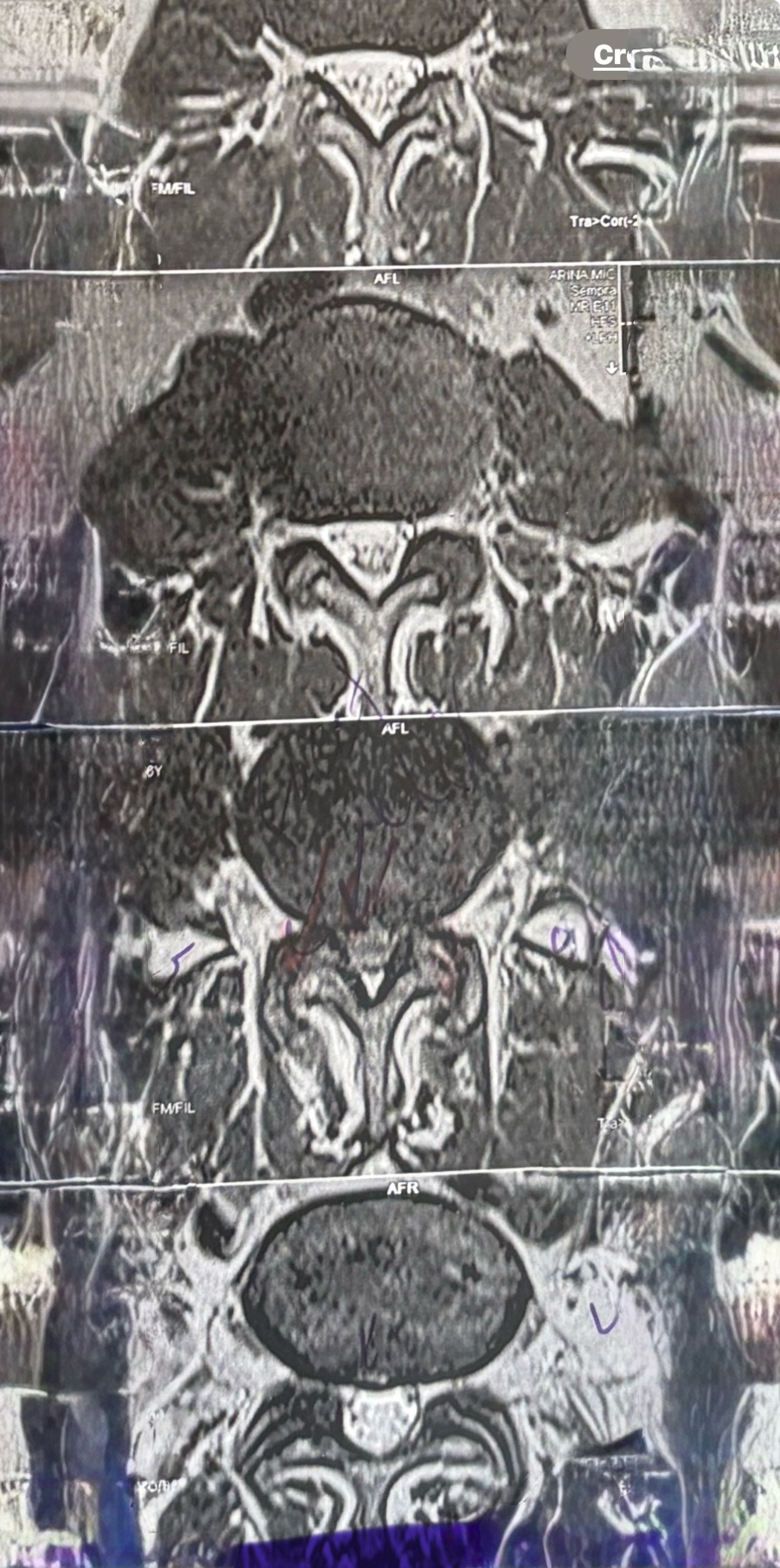
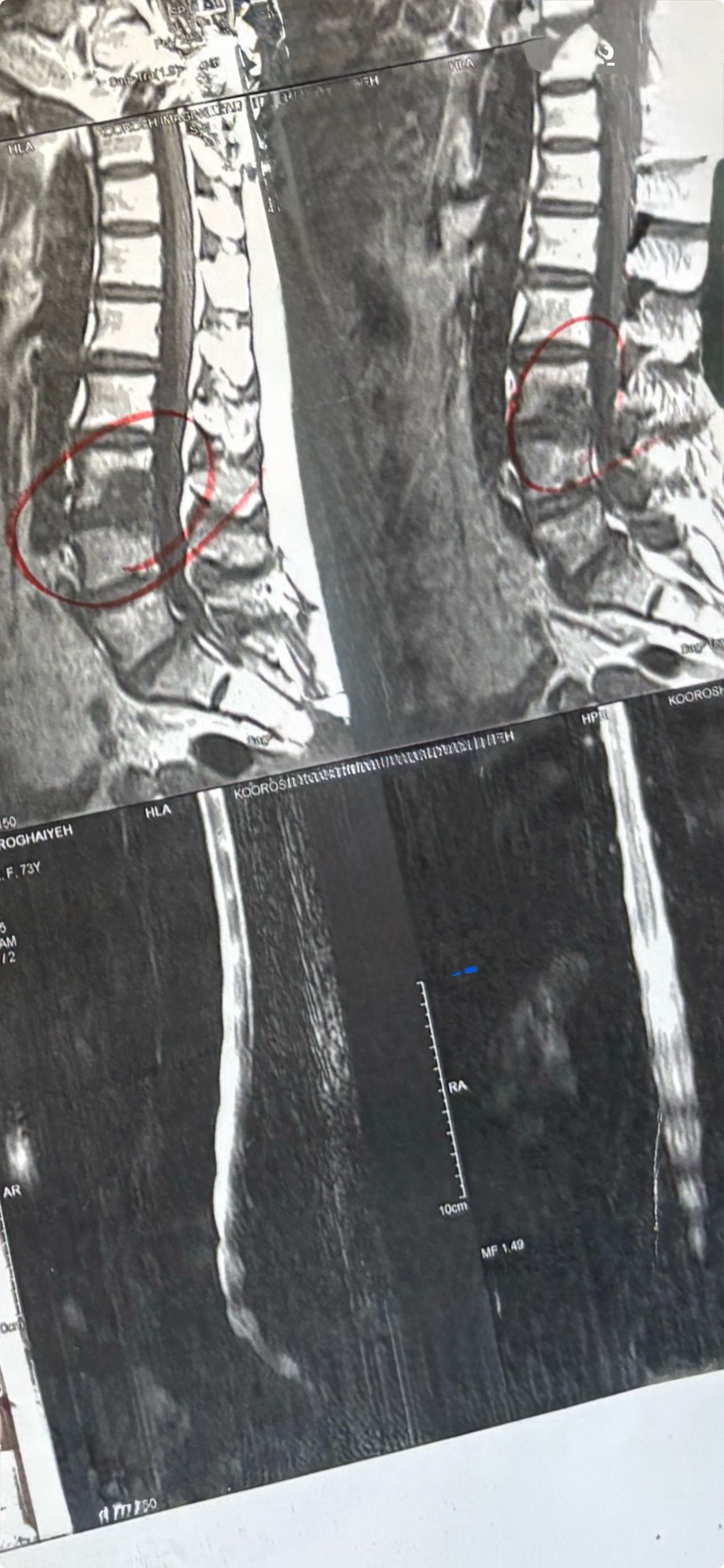
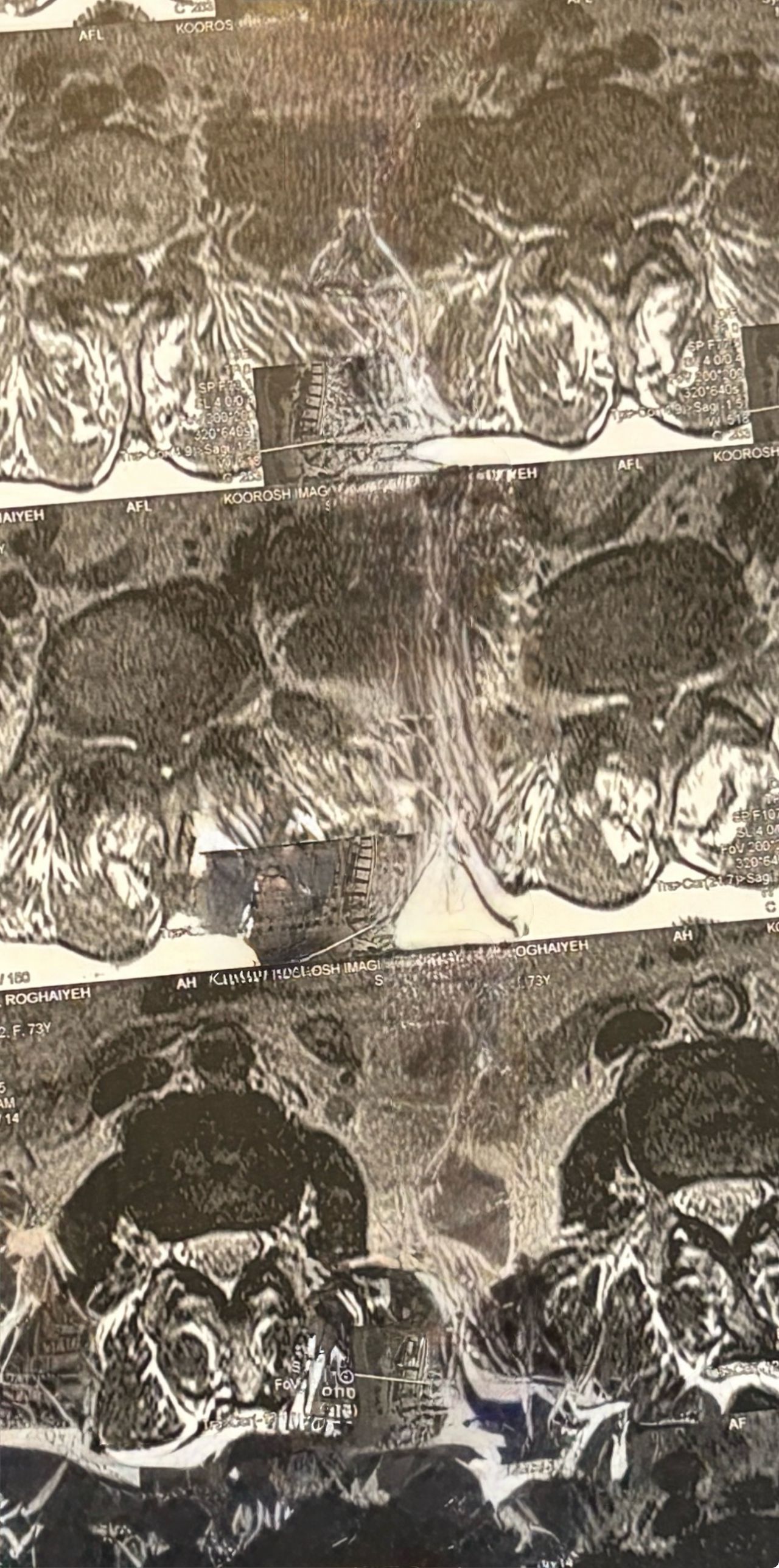
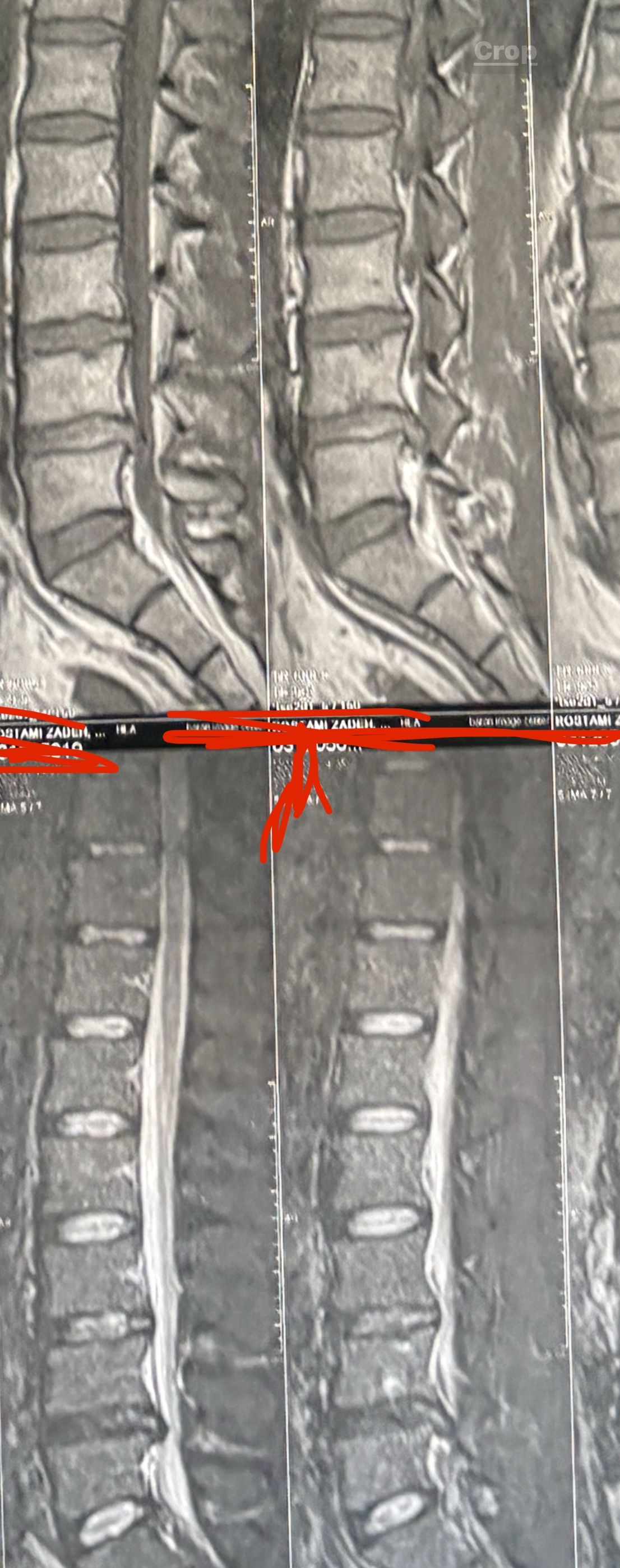
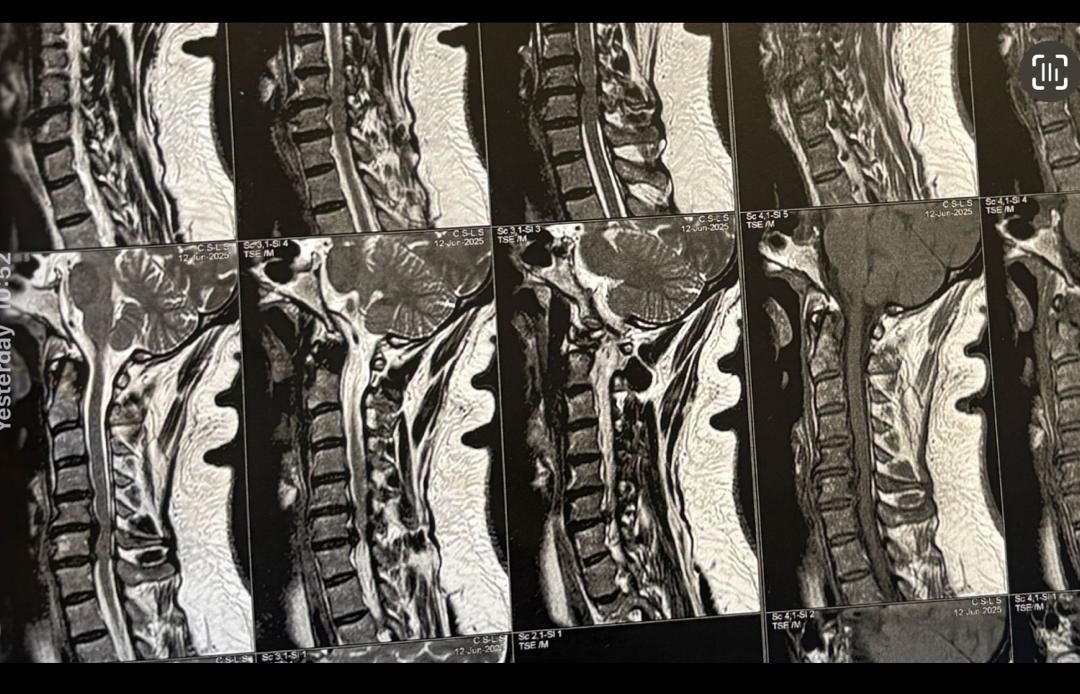
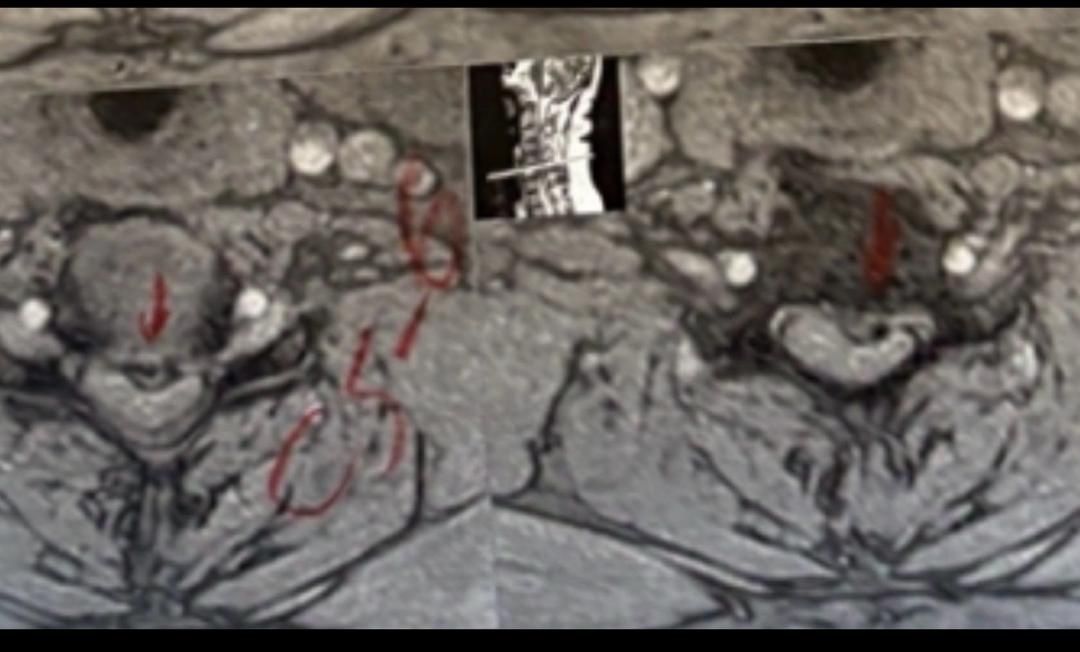
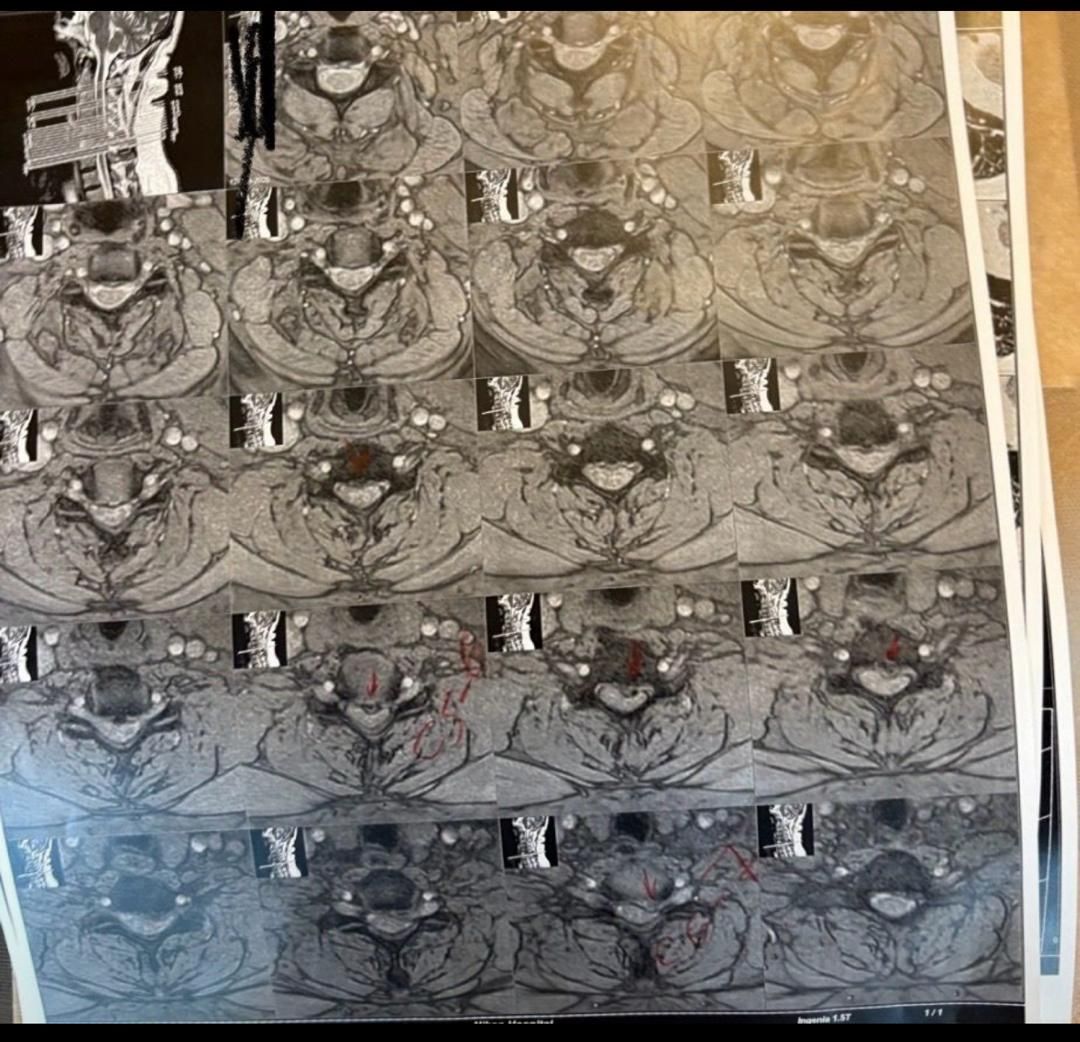
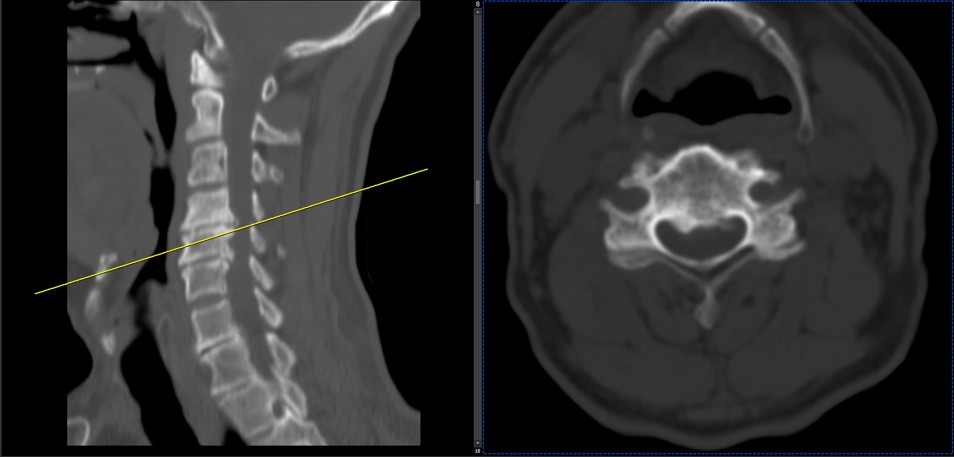
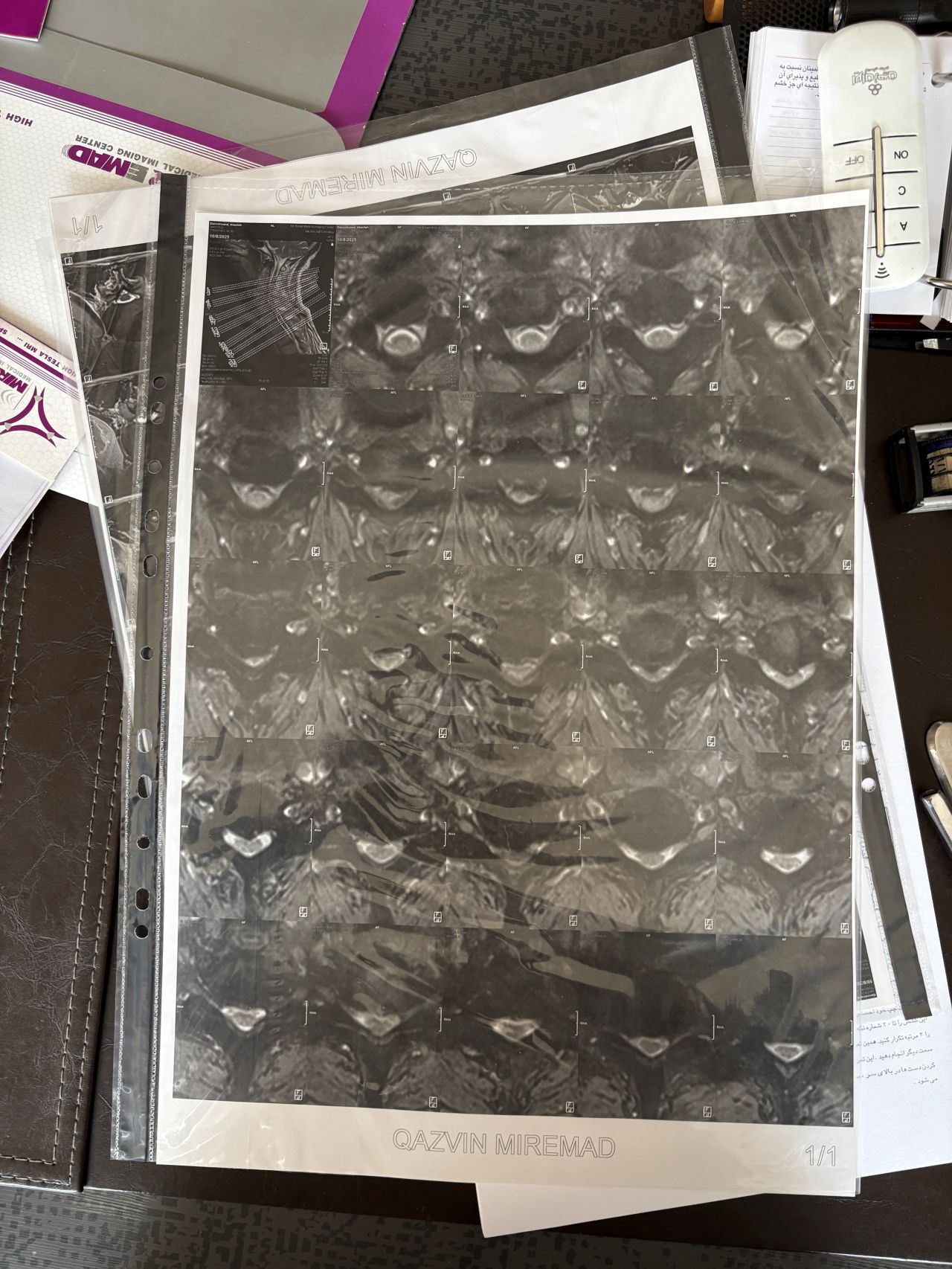
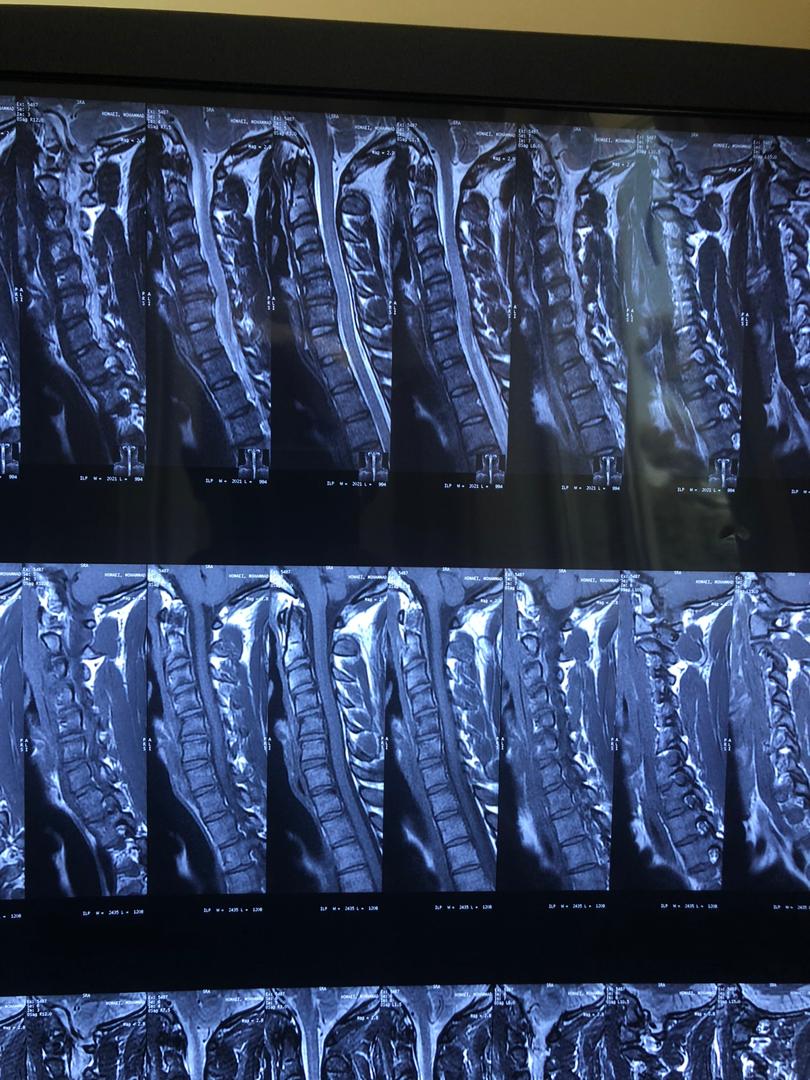
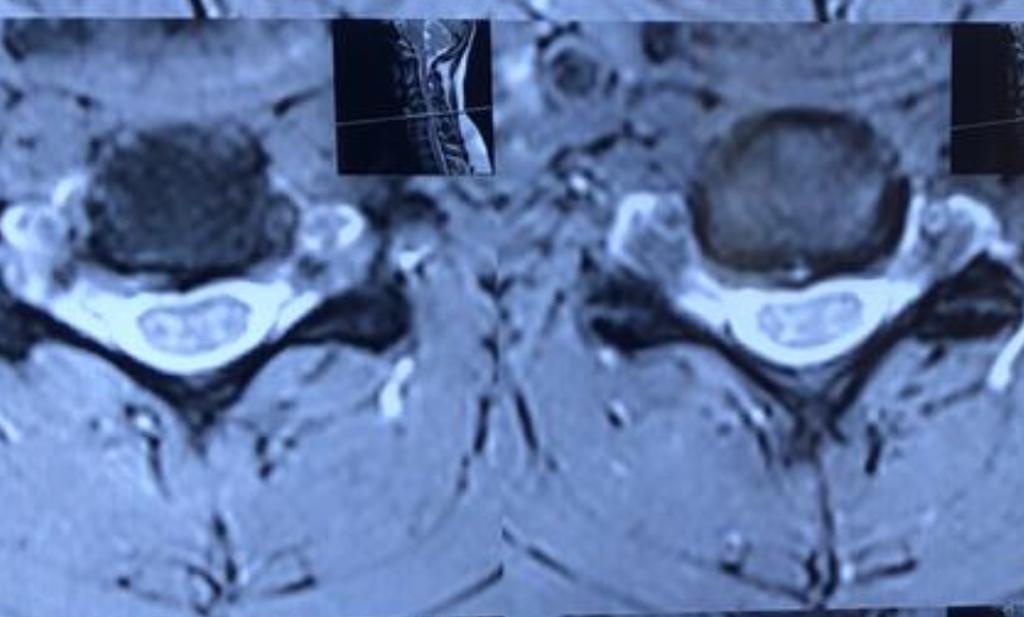
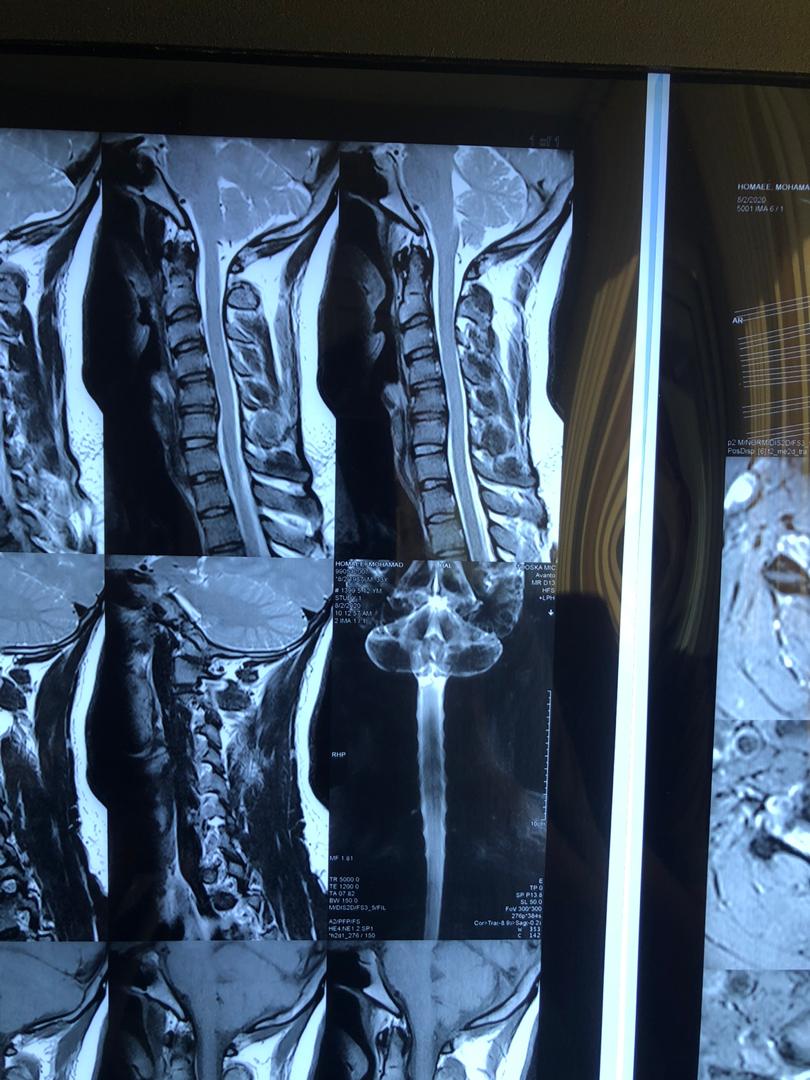
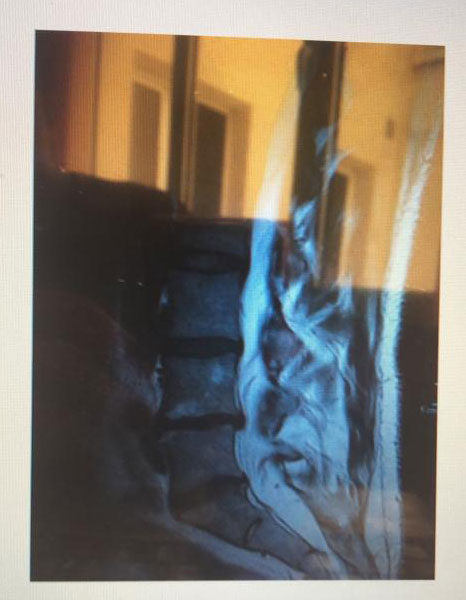
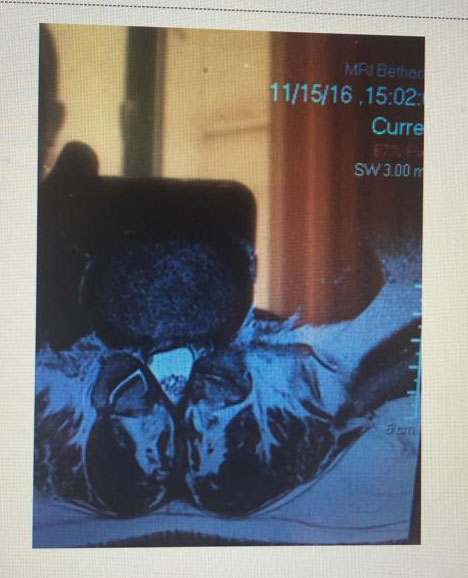
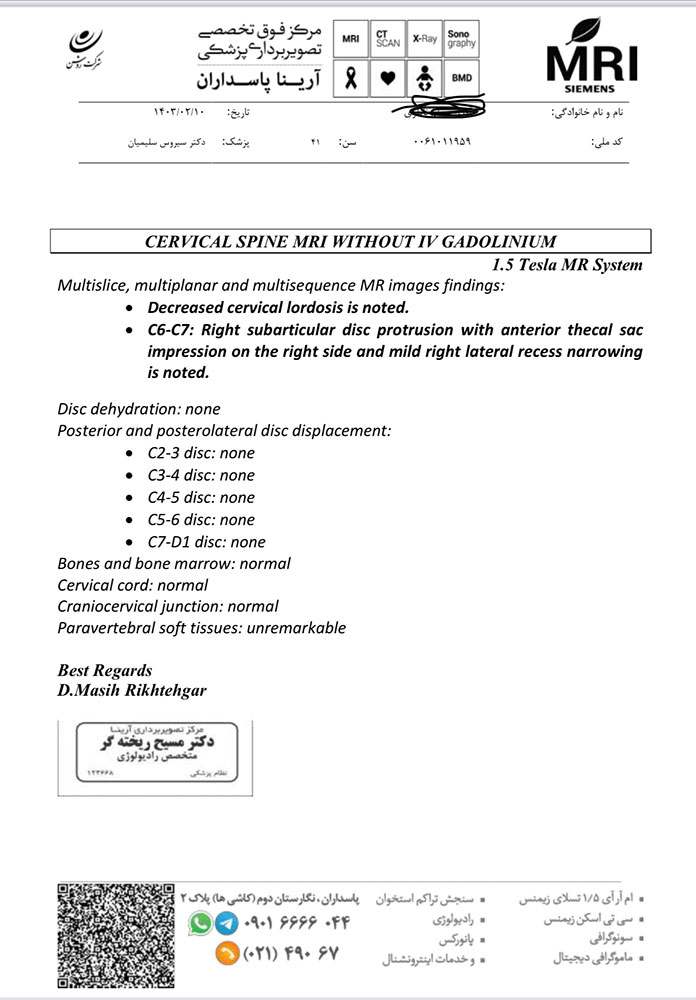
41 years old man presented to my clinic in October 2023 with acute and sever R neck pain with radicular pain to his R upper extremity along C6 dematom since 2 weeks ago. Examination didn’t show any upper motor signs. Was suggested urgent surgery
I ordered EMG/ NCV : showed mild R C6, C7 irritation without any active axonal loss

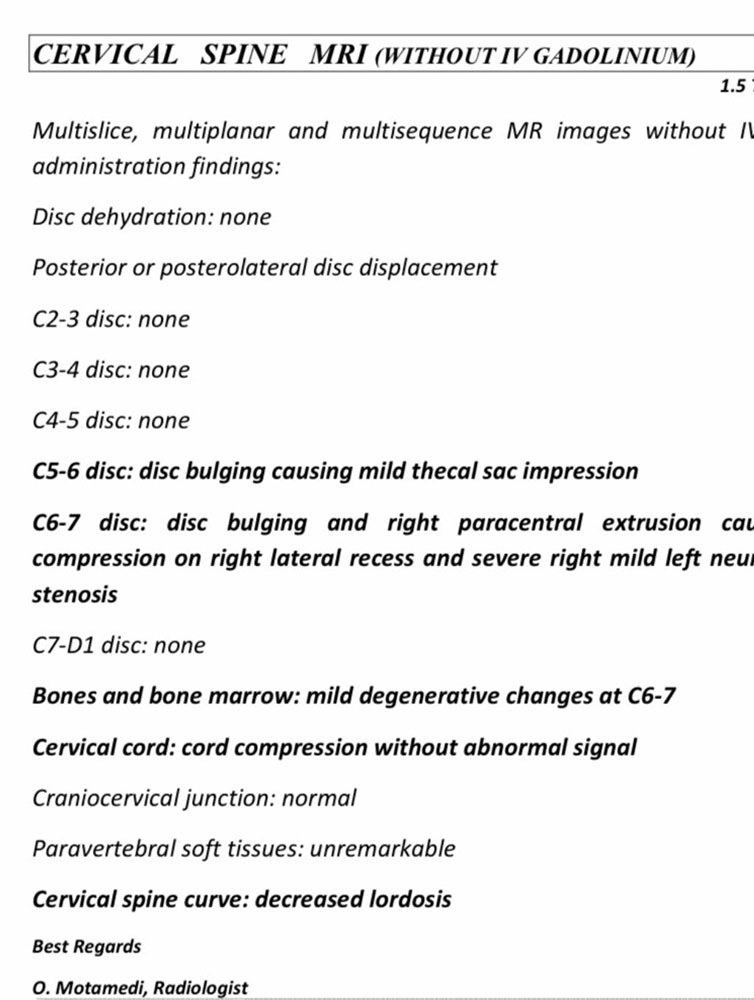

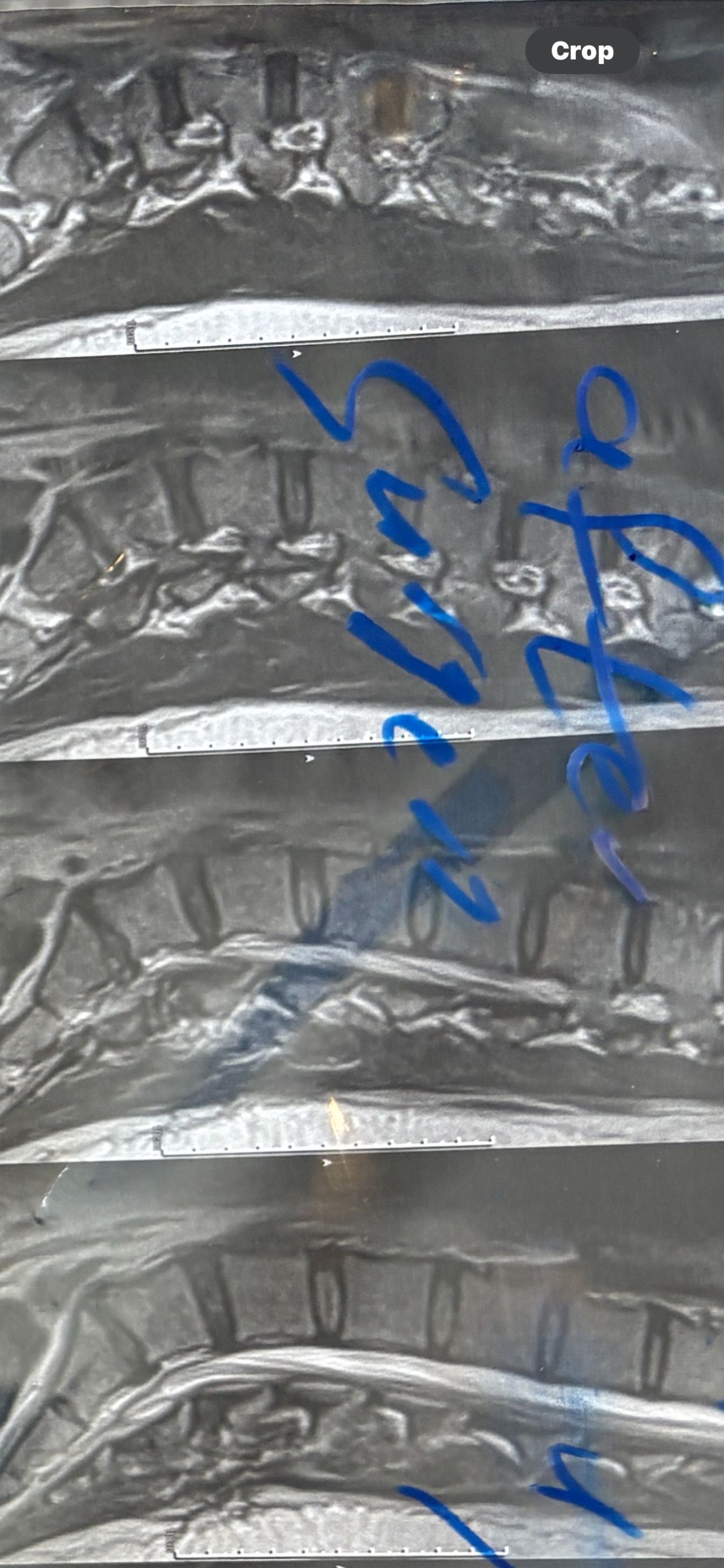
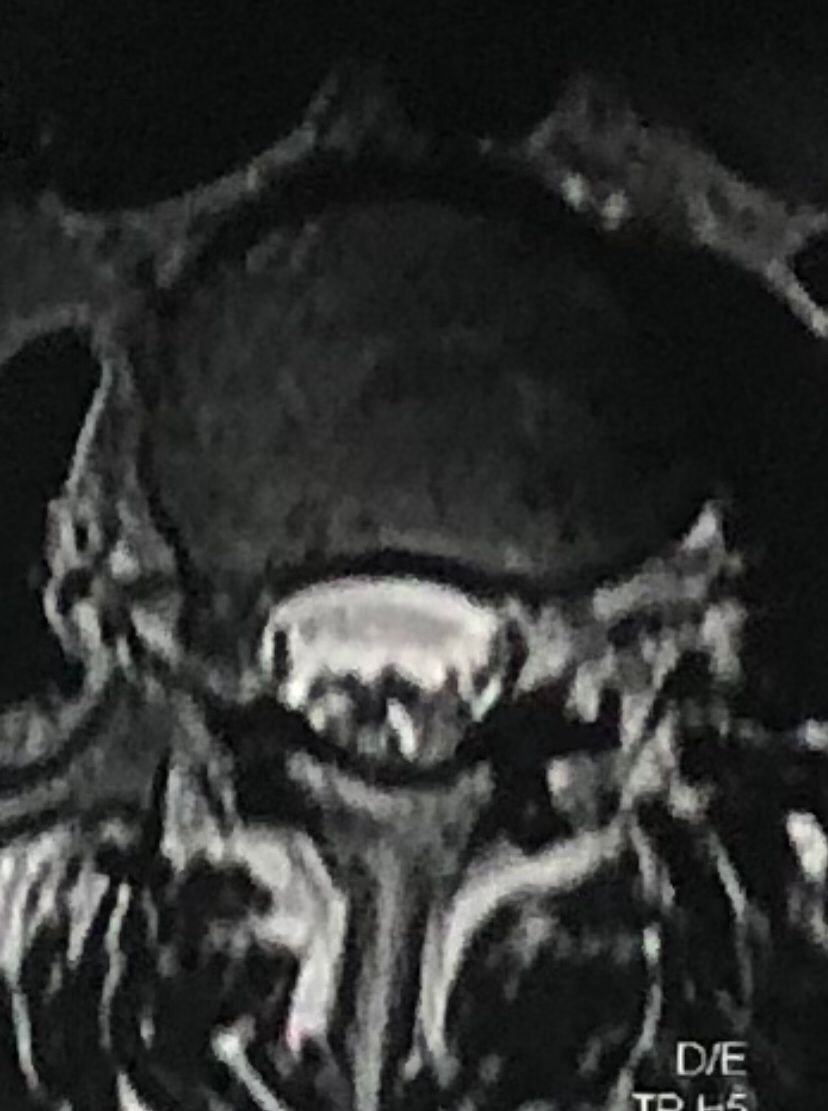
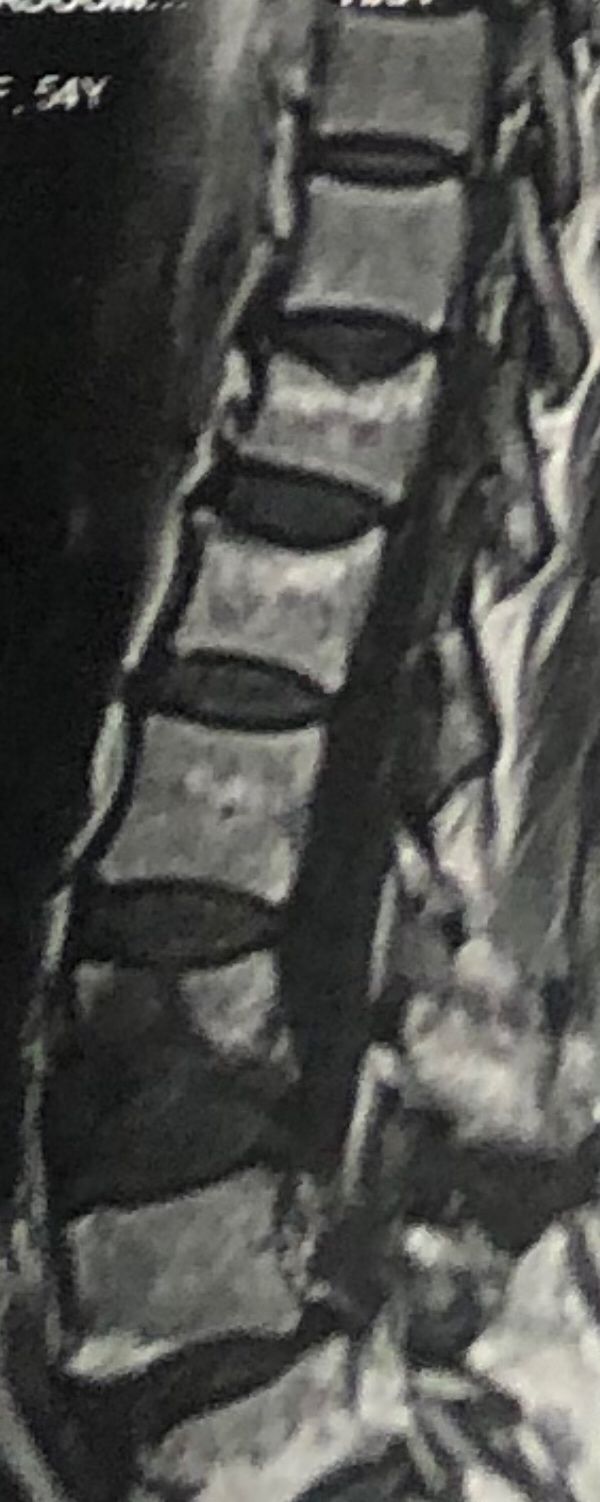
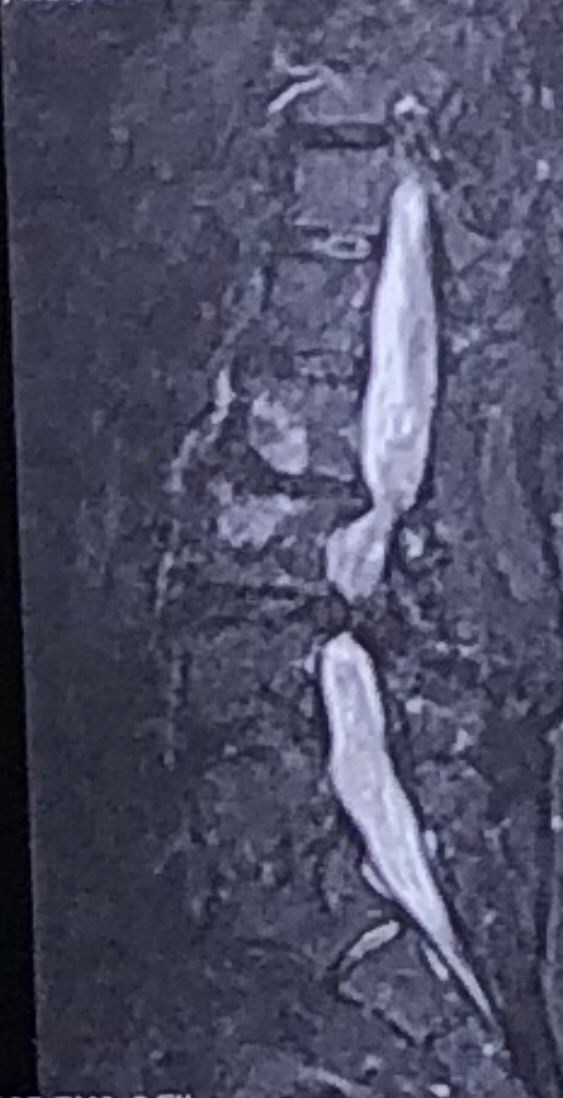
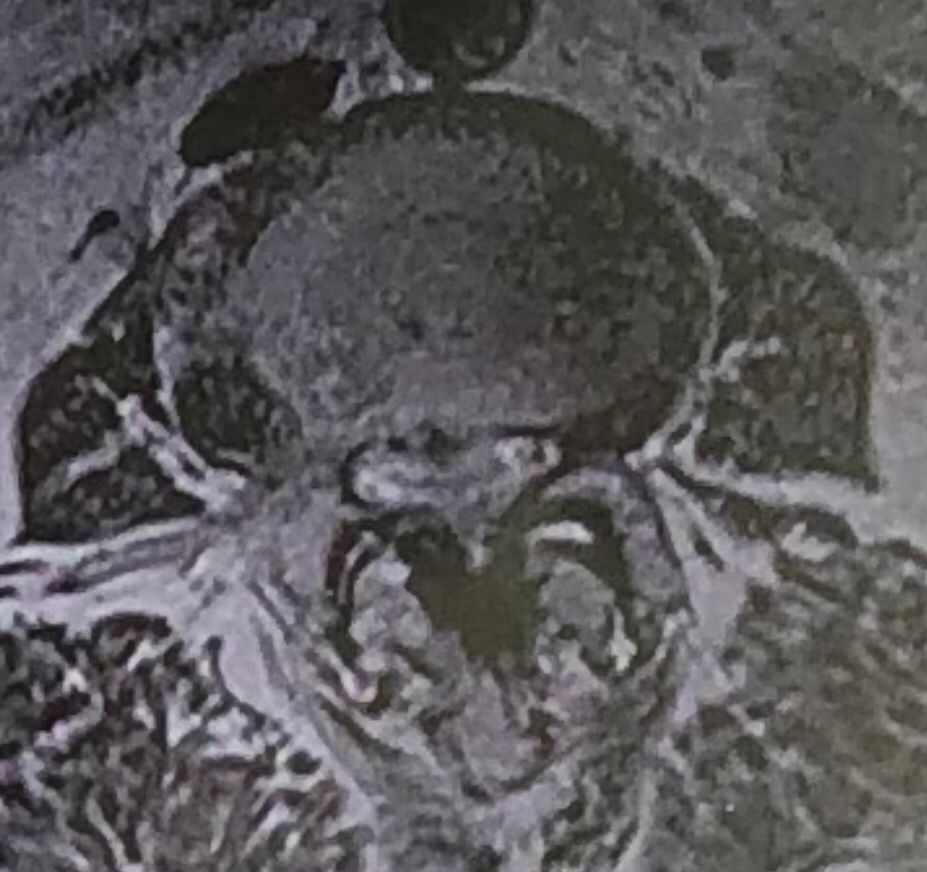
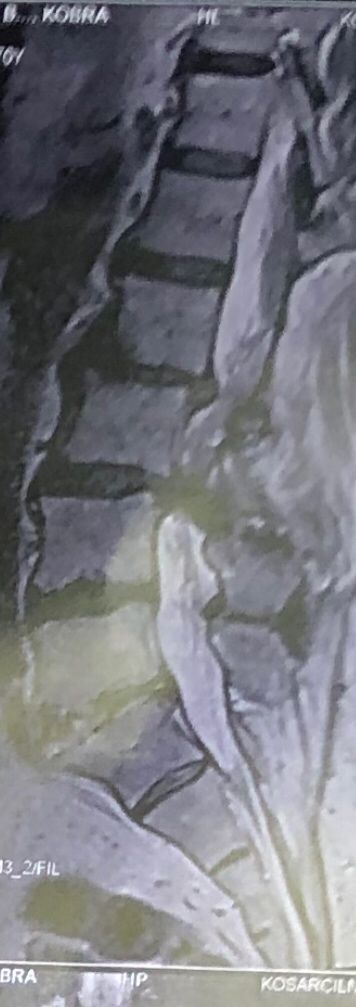
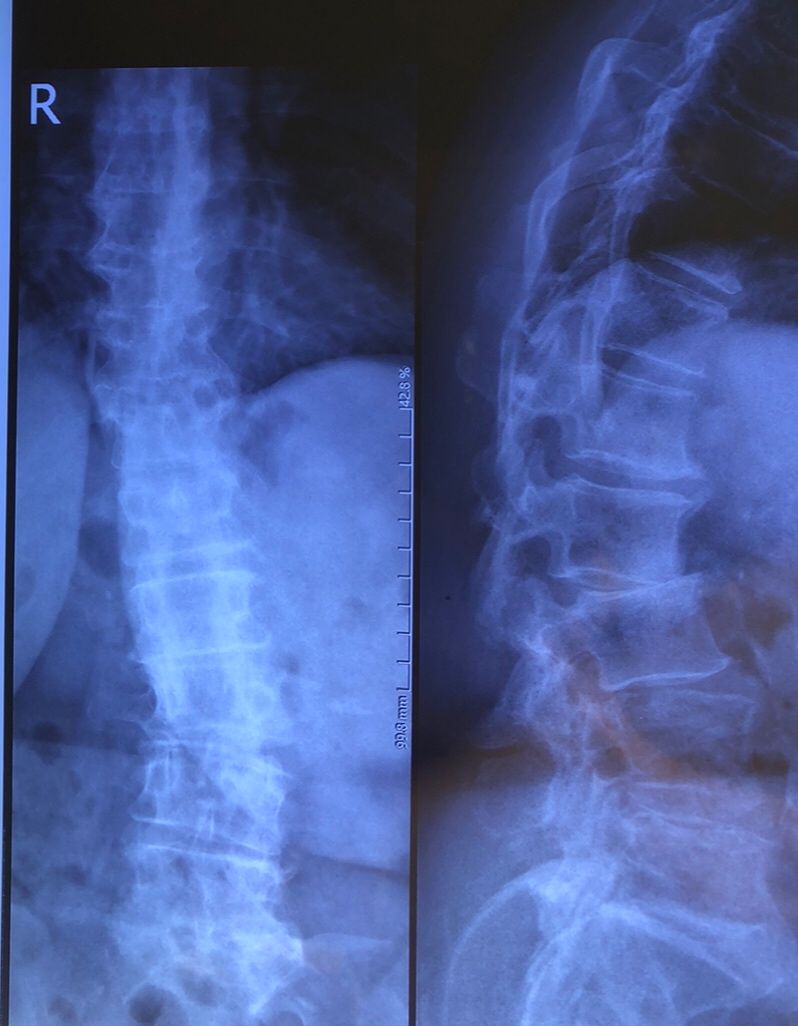
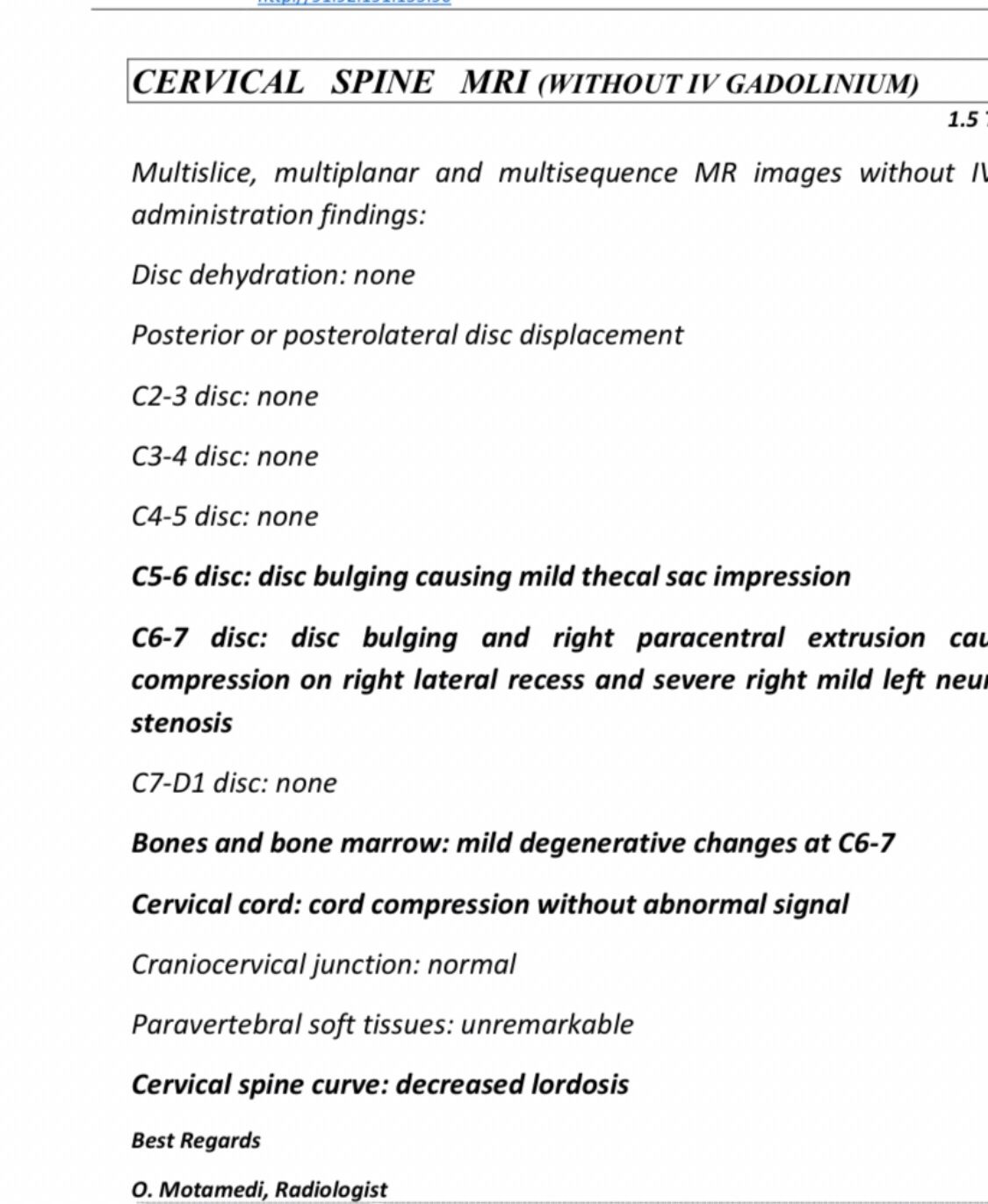
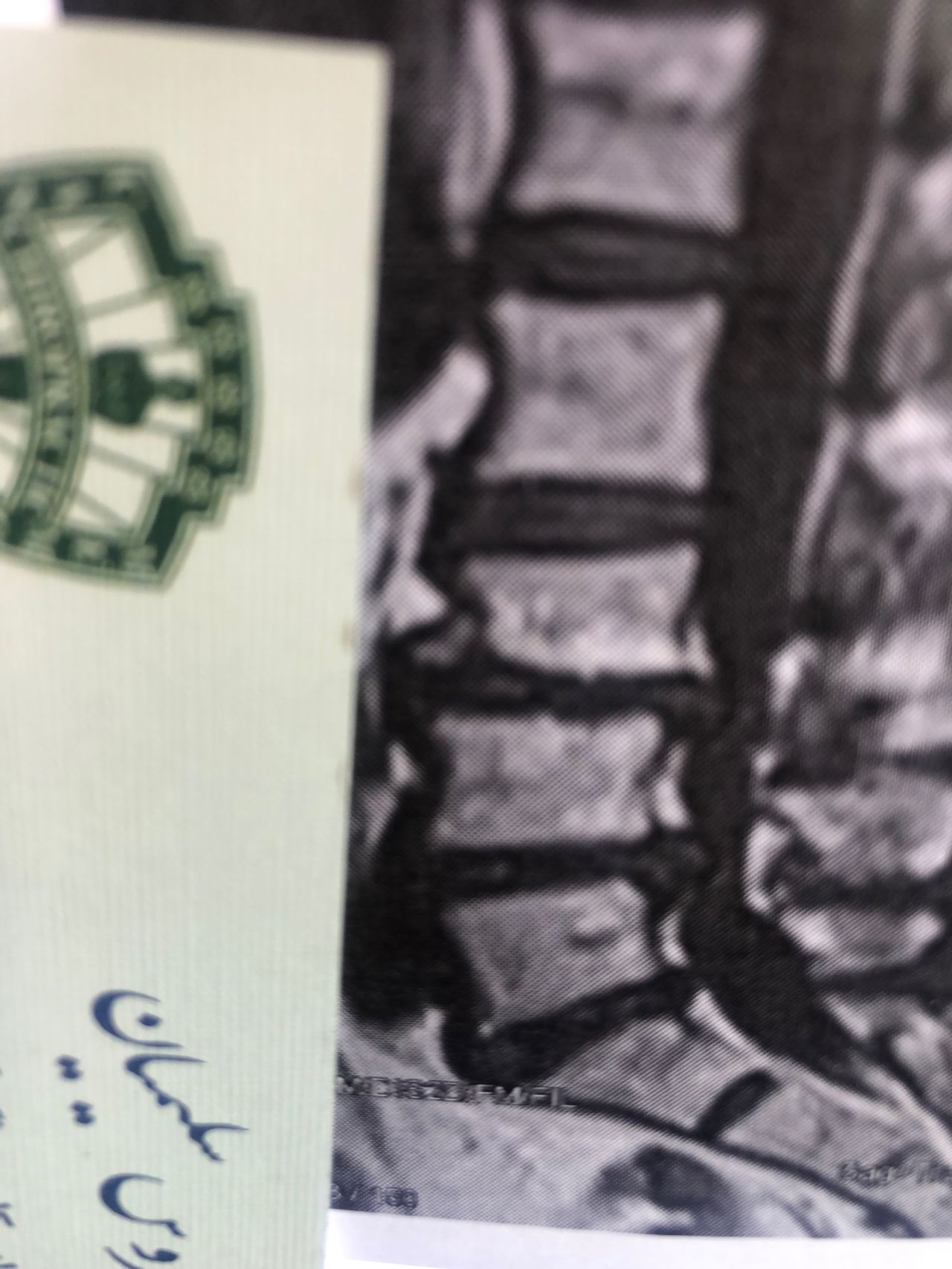
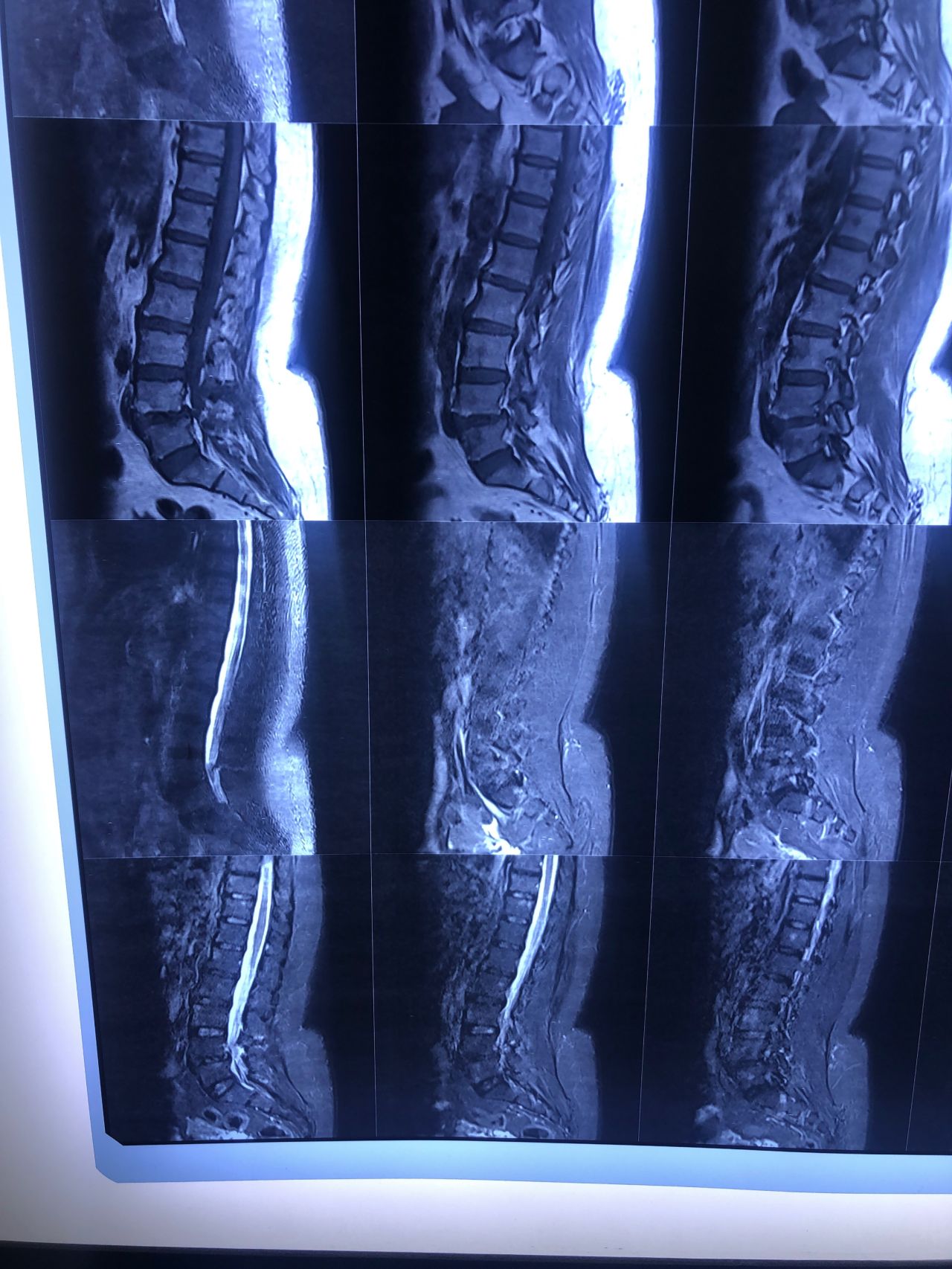
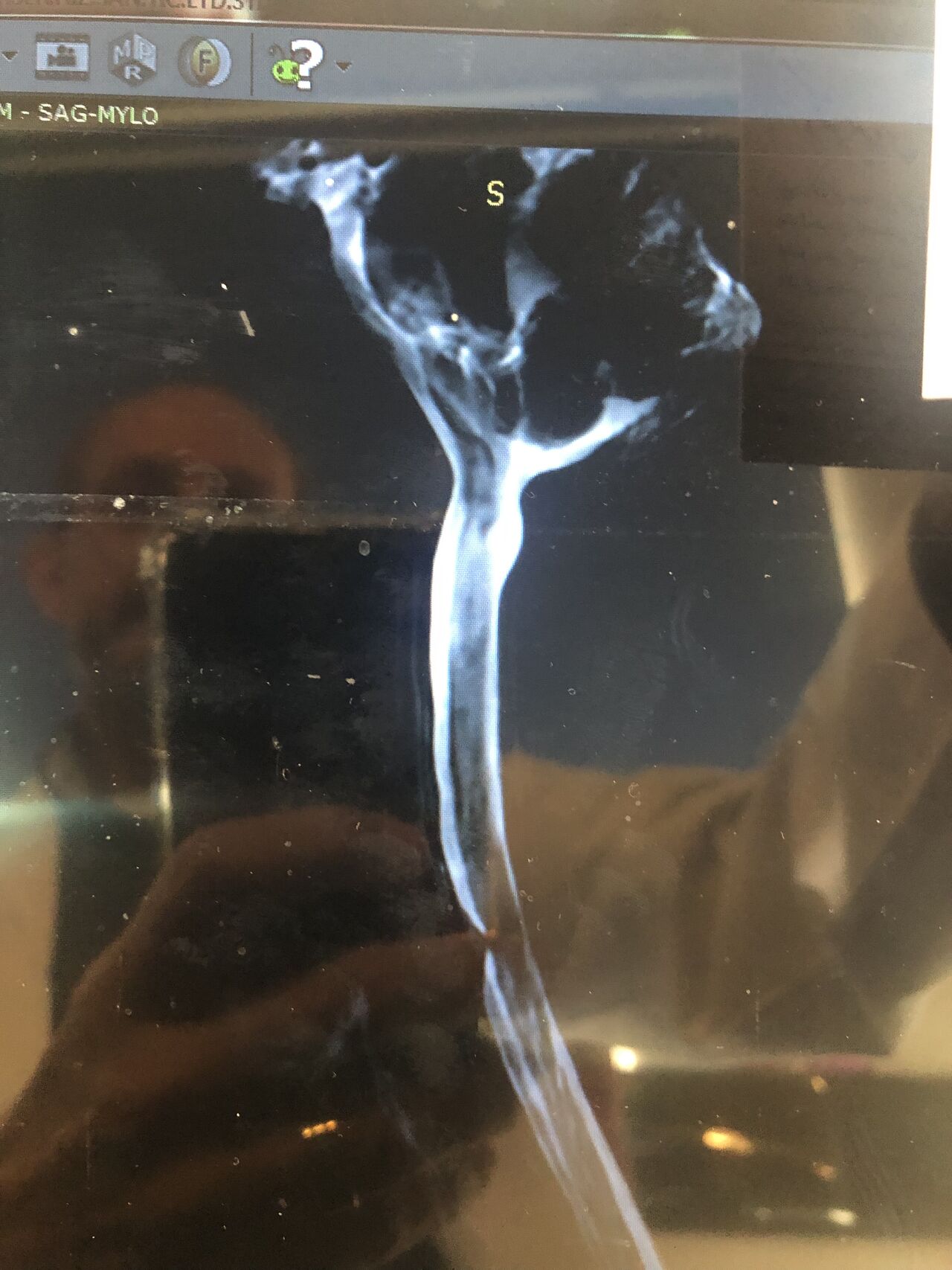
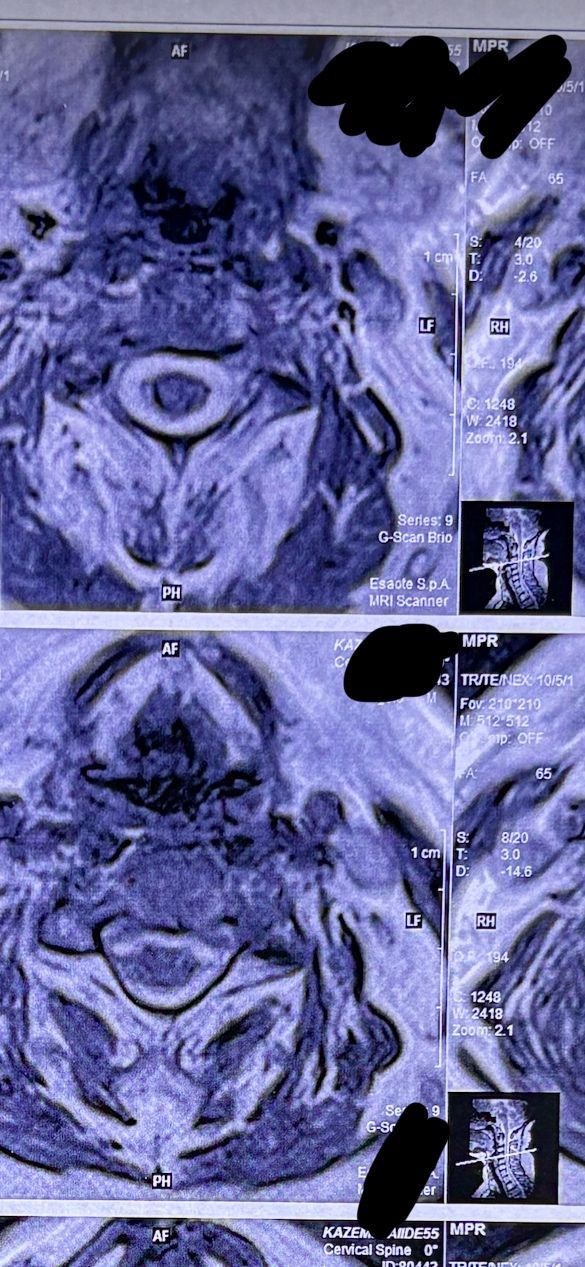
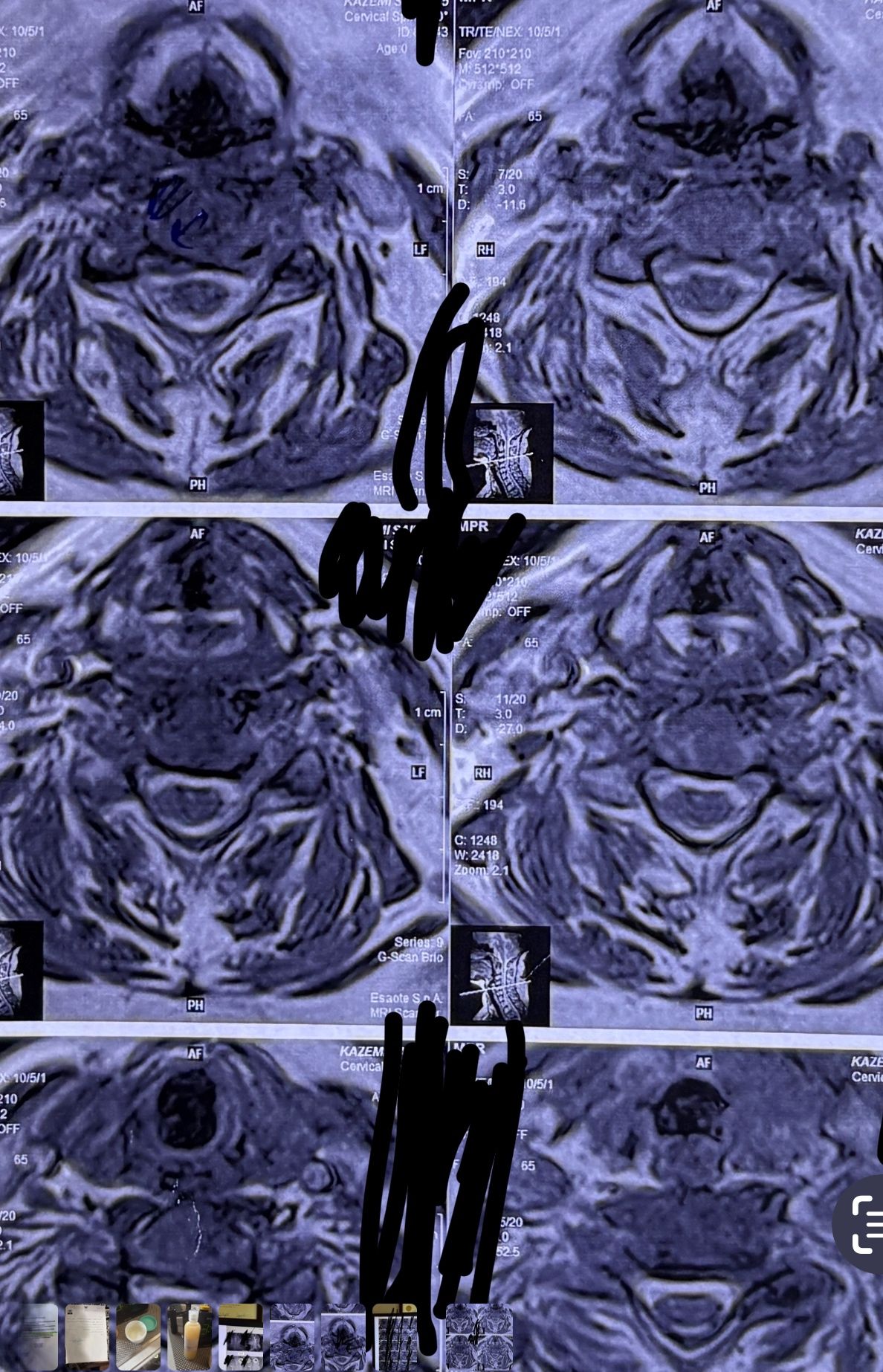
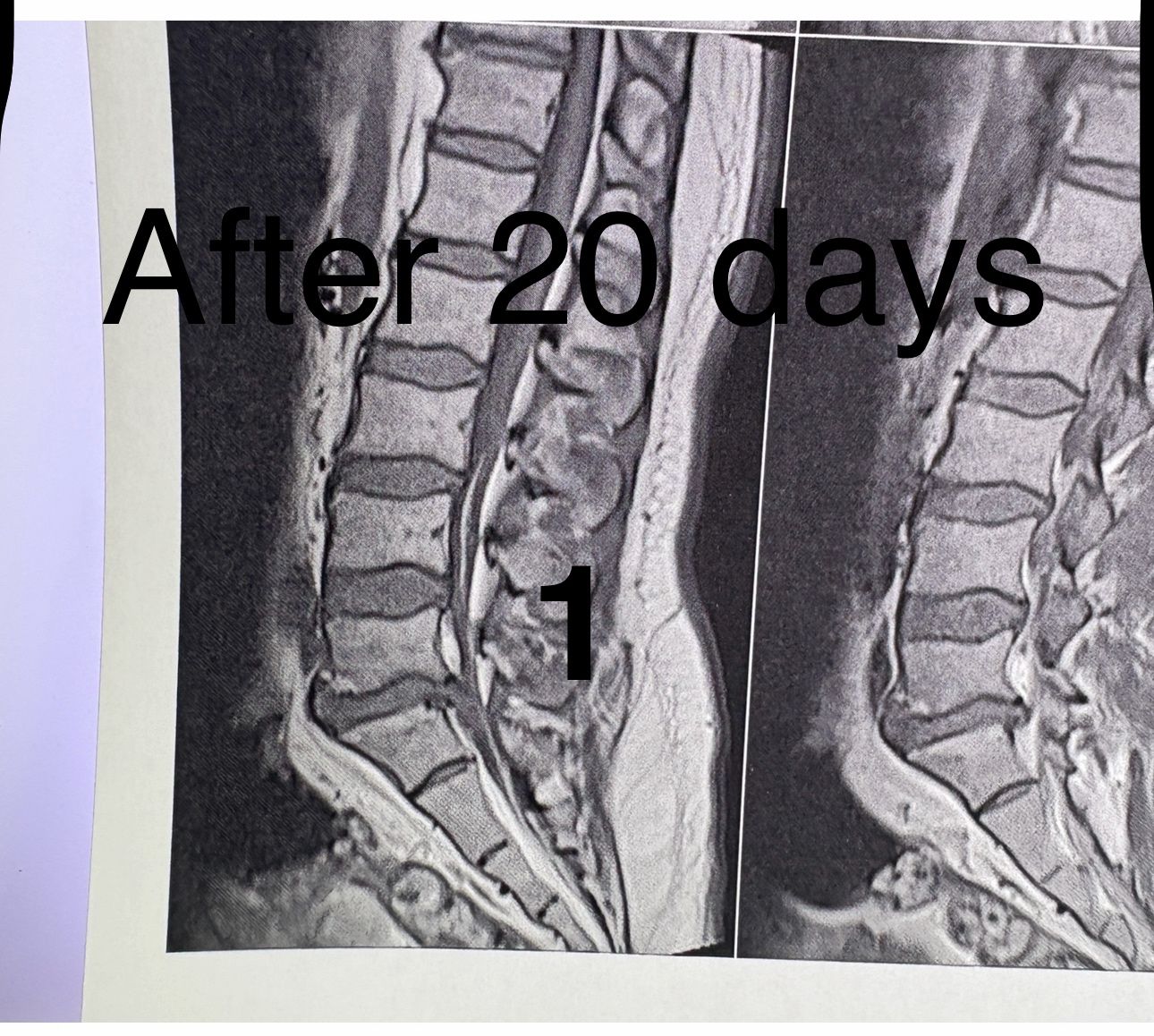
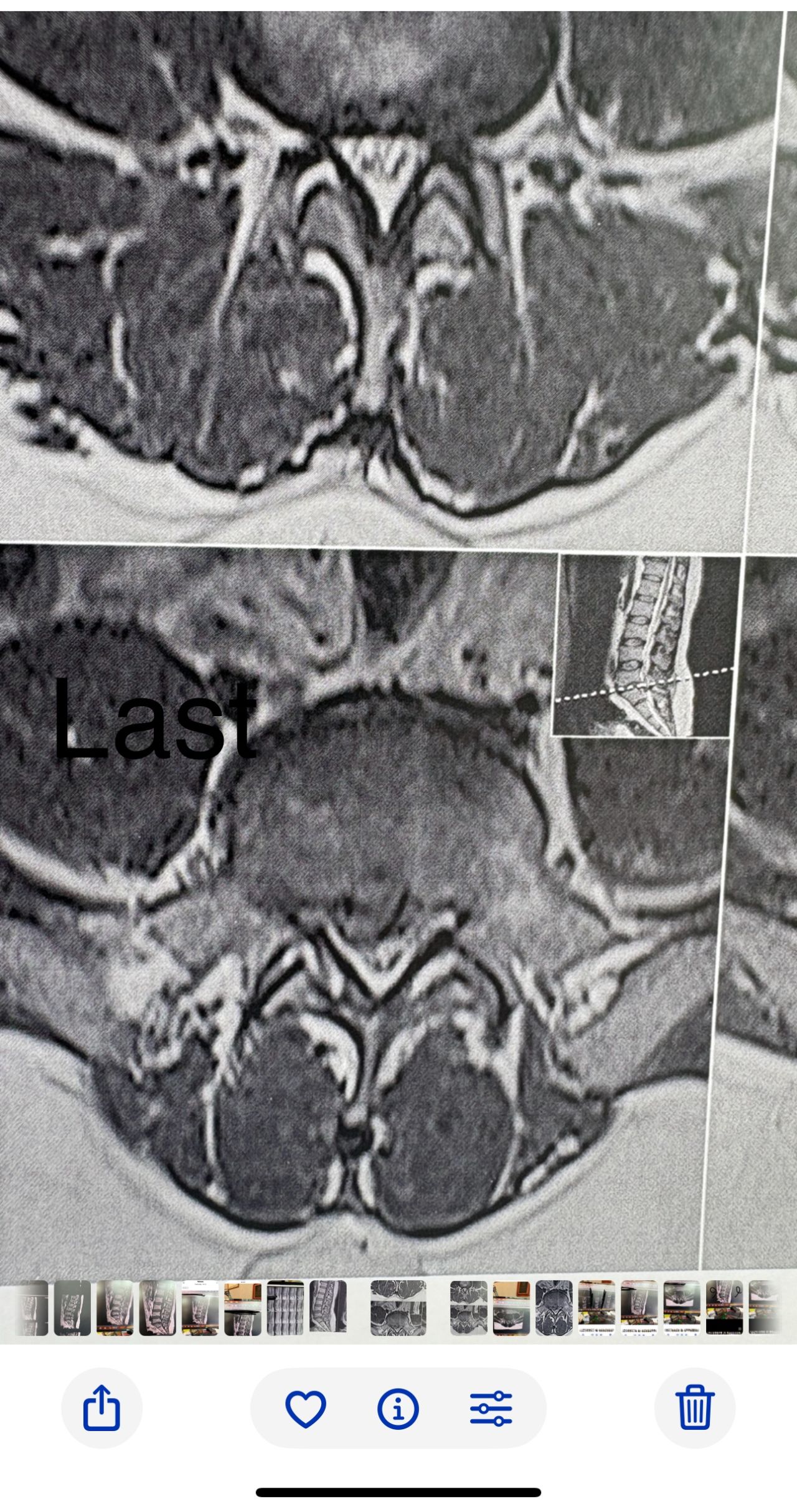
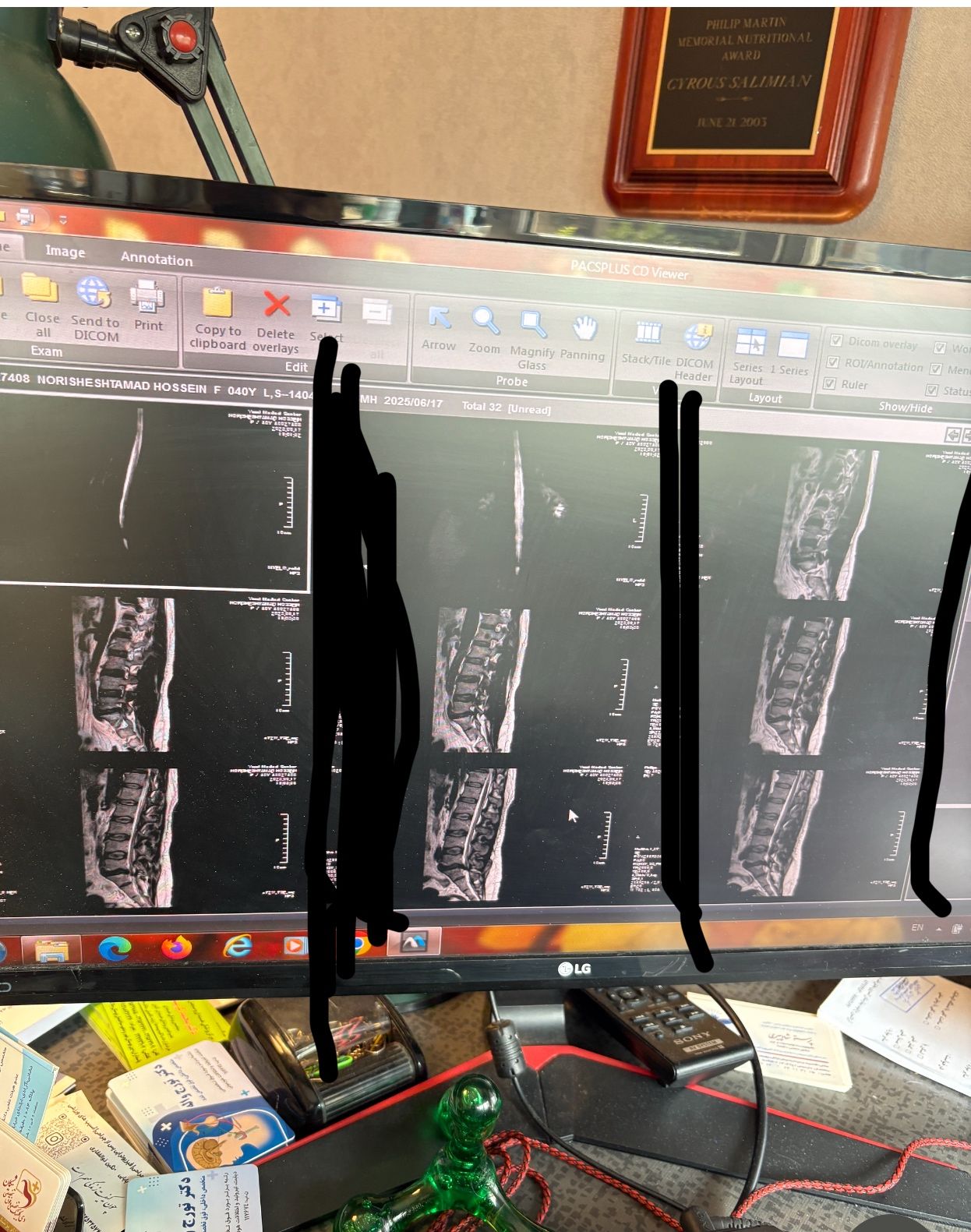
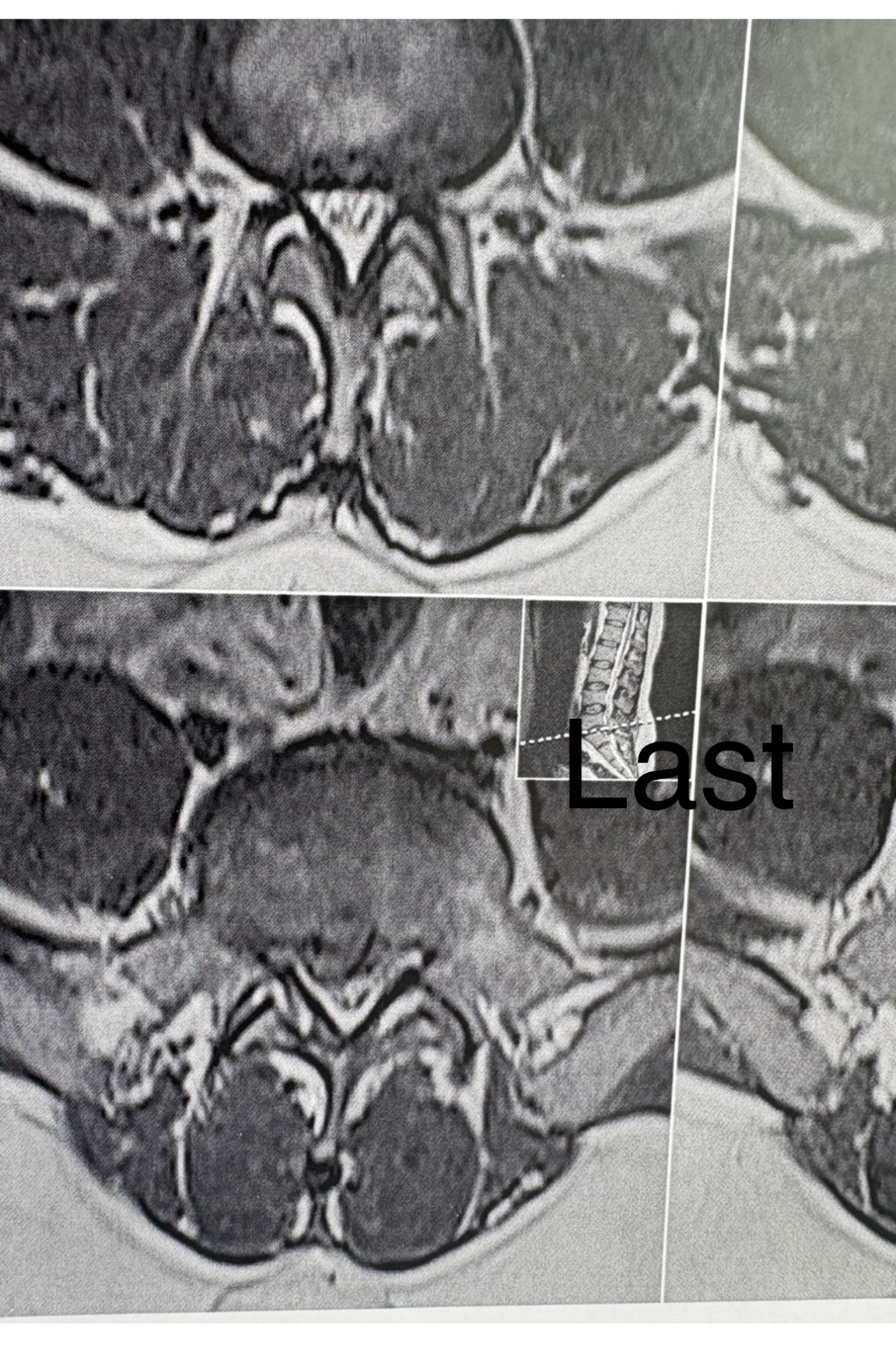
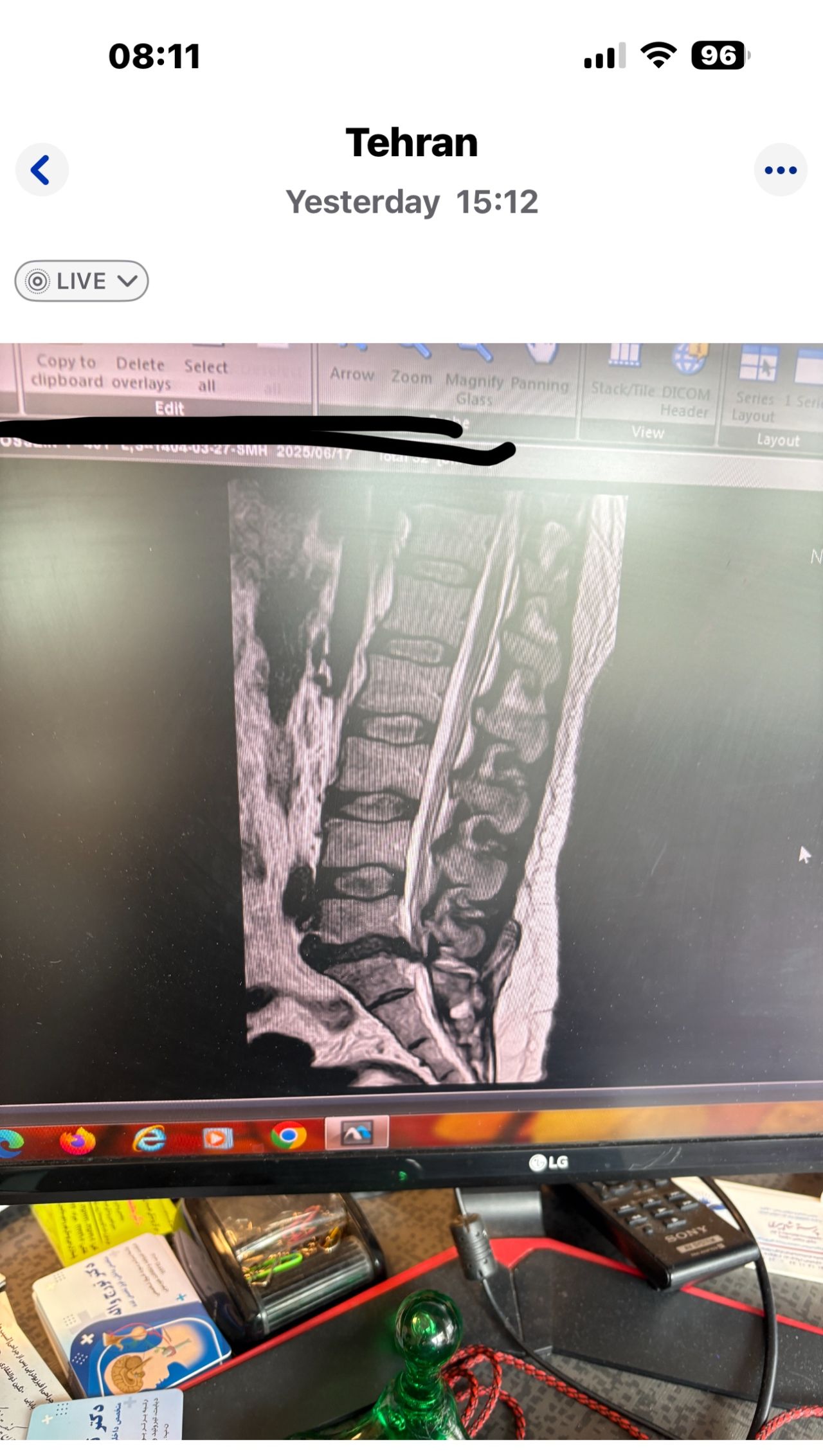
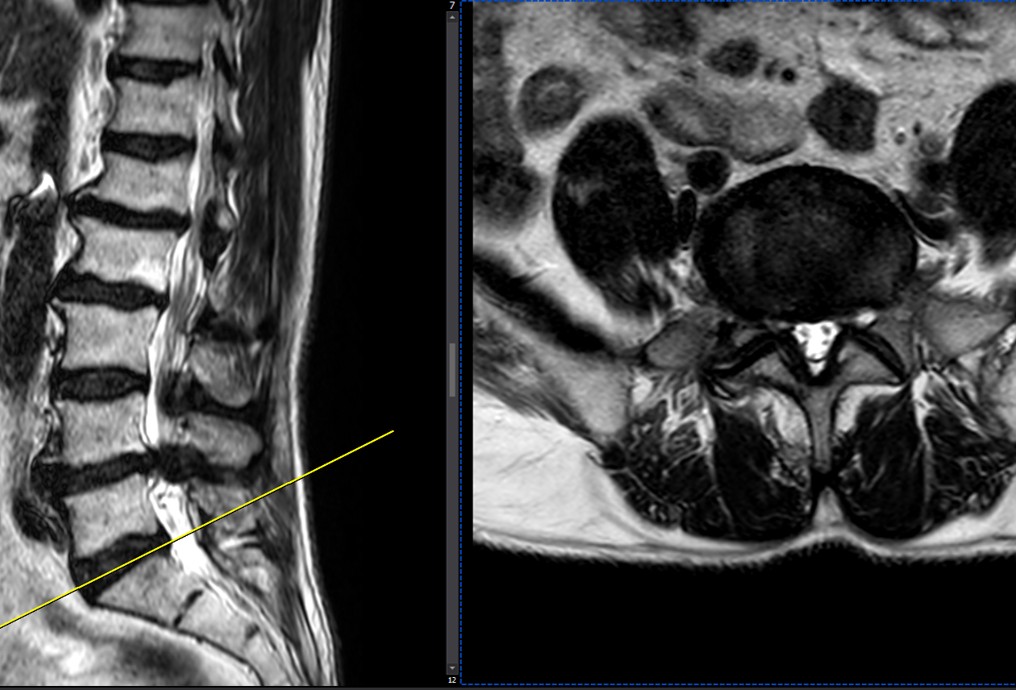
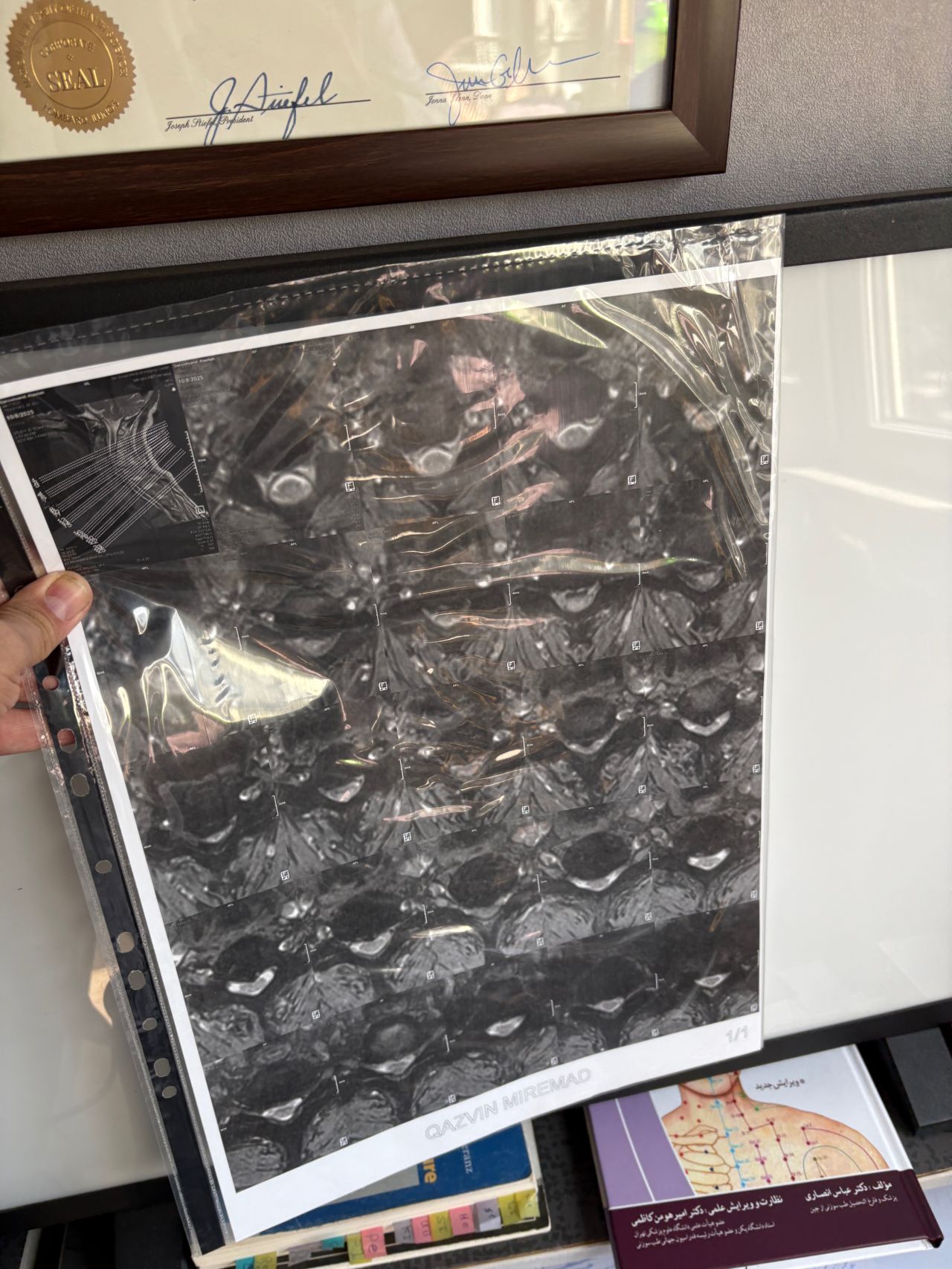
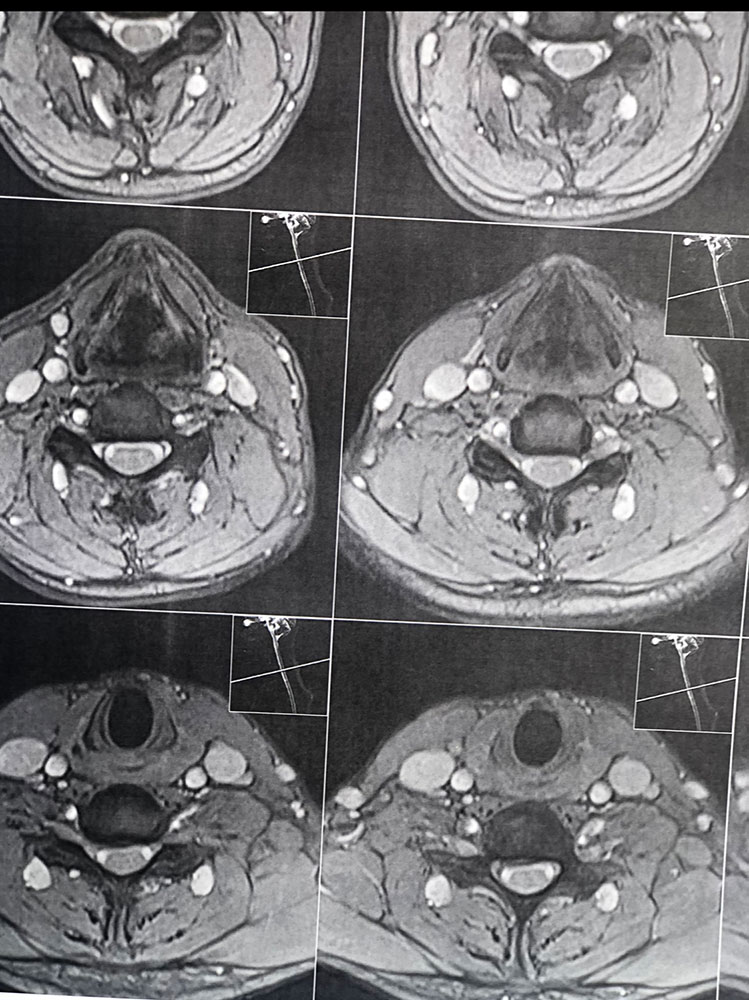
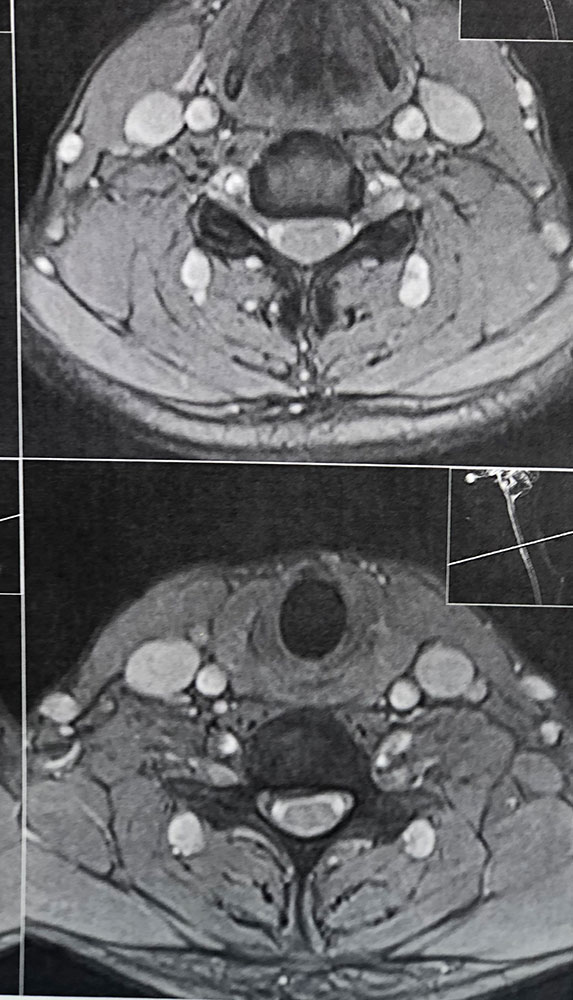
In his MRI was reported R. para R. IVF Massive extrusion. I decided to control his pain and manage this patient with reevaluation of patient every other session. For 5 sessions i just used acupuncture and laser and IFC and mild adjustments to his R. T3-T7 and mild arthosteem to above and below involved segment. Cervical adjustment considered contraindicated for this patient. From session 6th- 8th i started to use mild/gentle cervical decompression. He used soft cervical collar all the time. His pain decreased by 80 percent
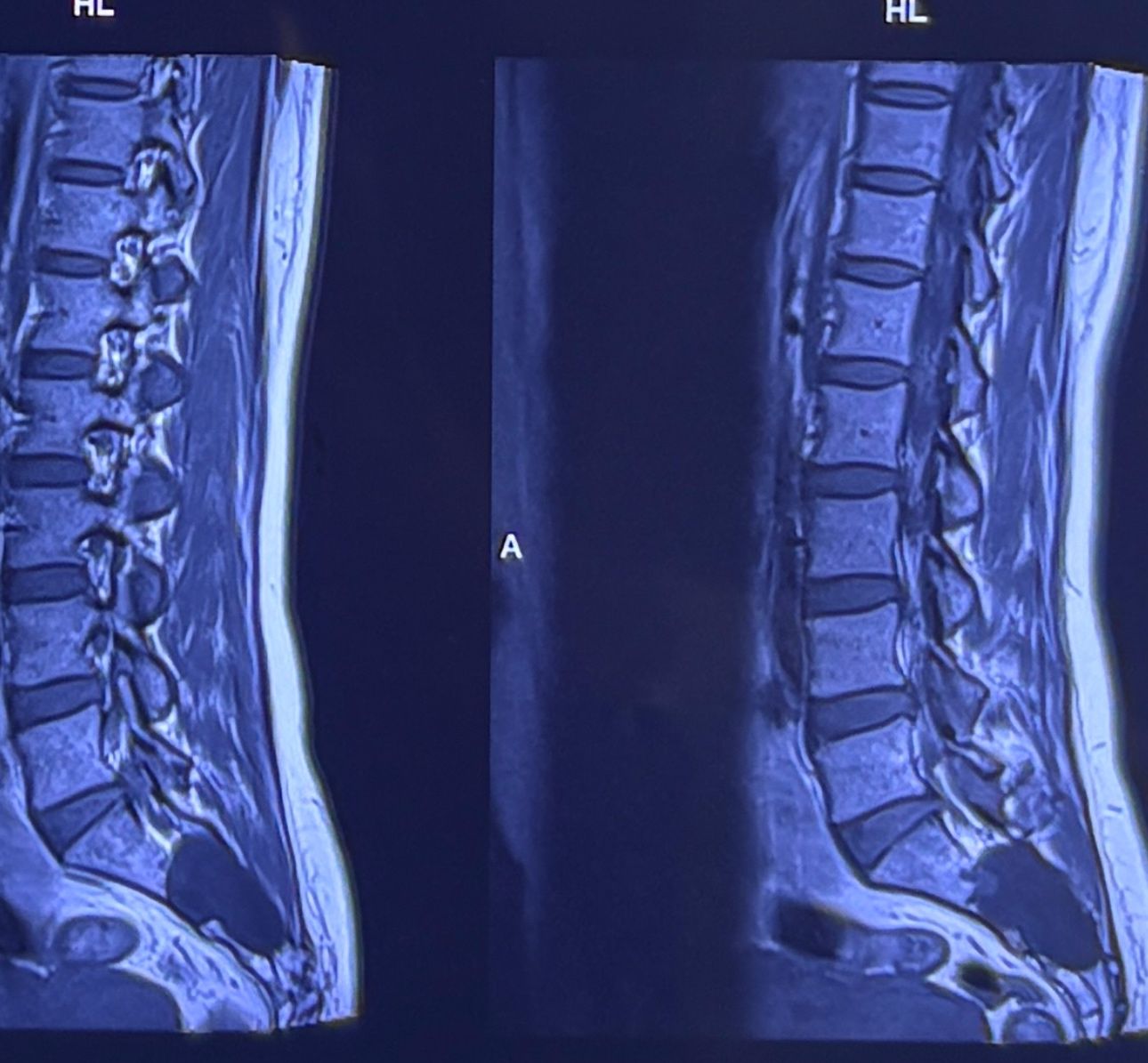
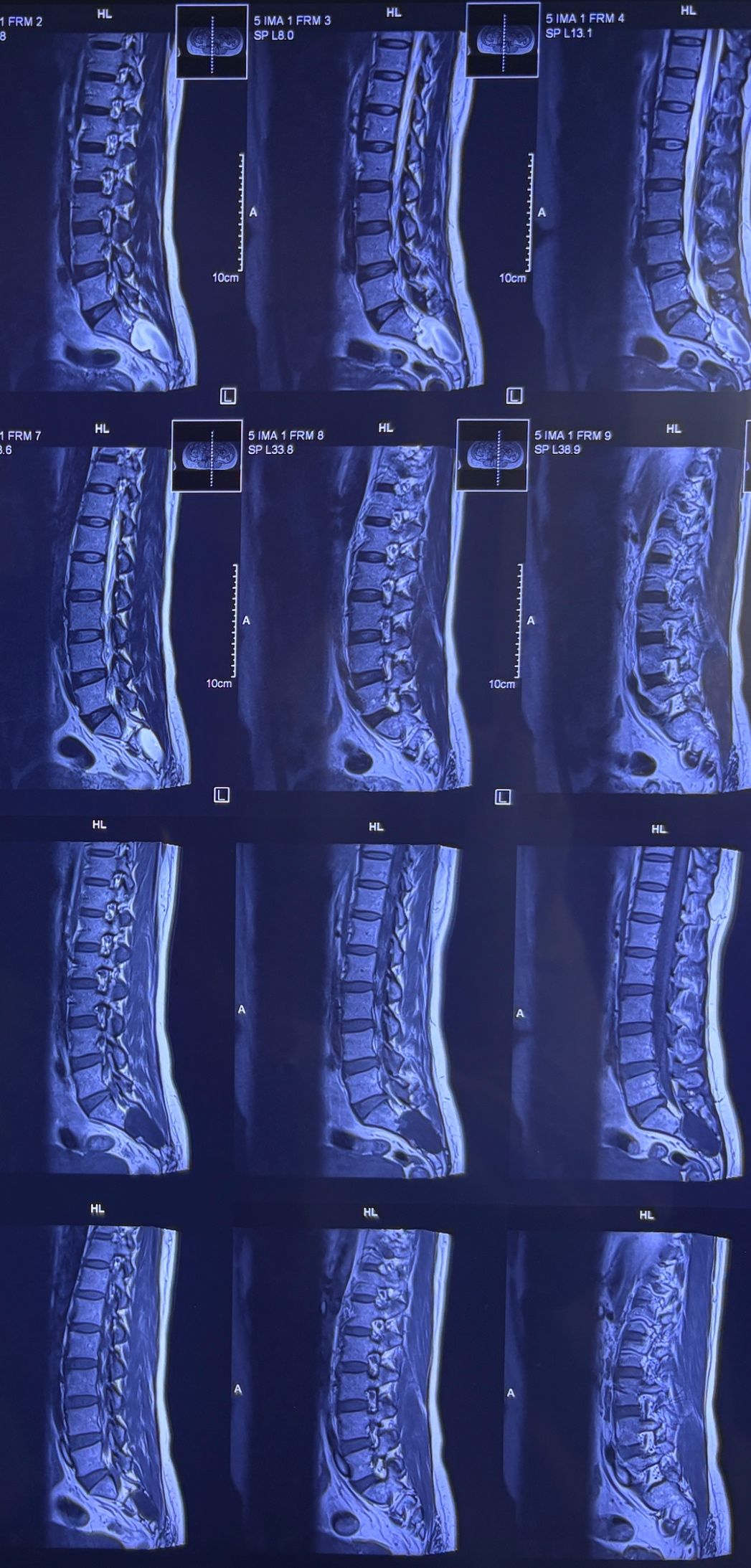
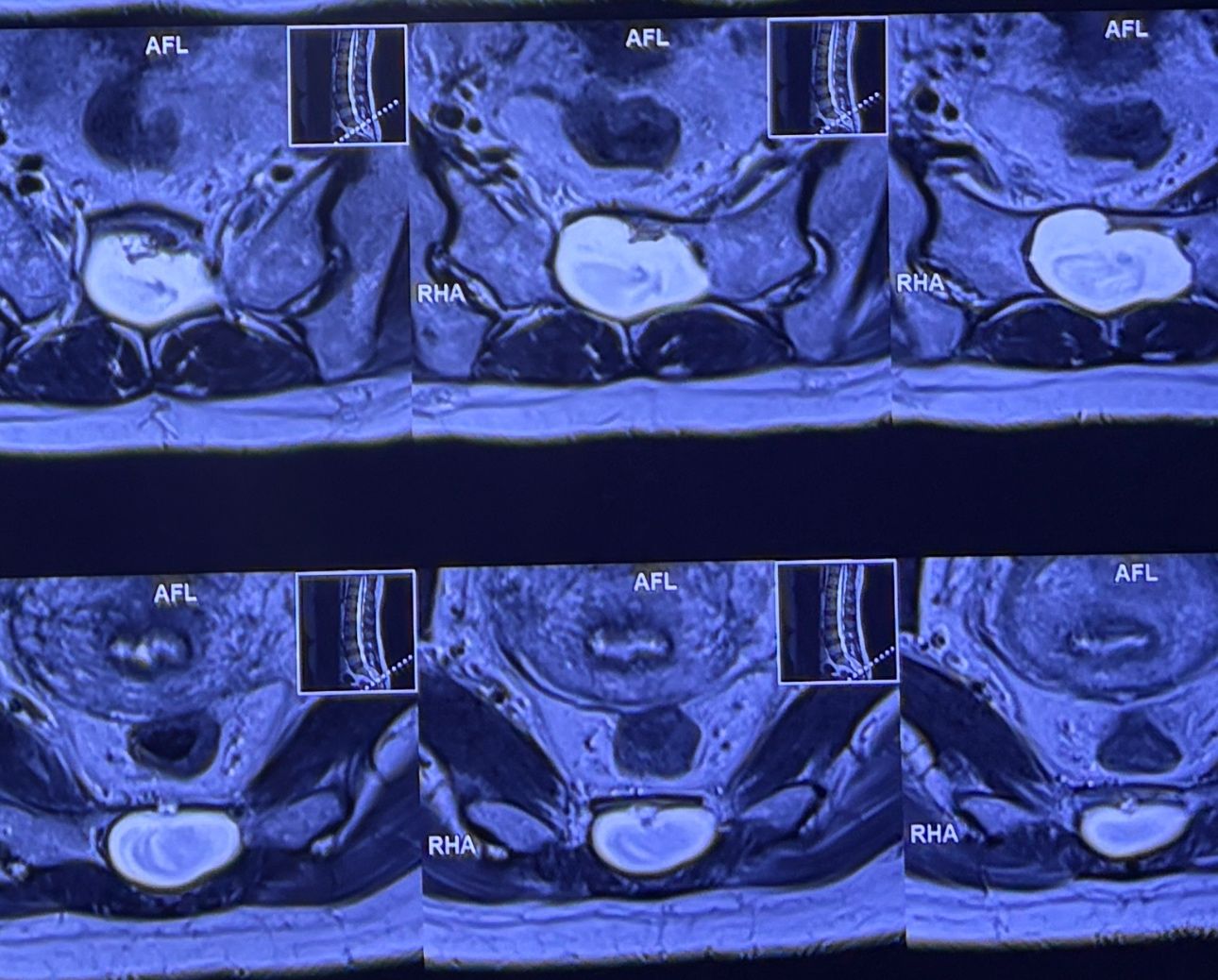
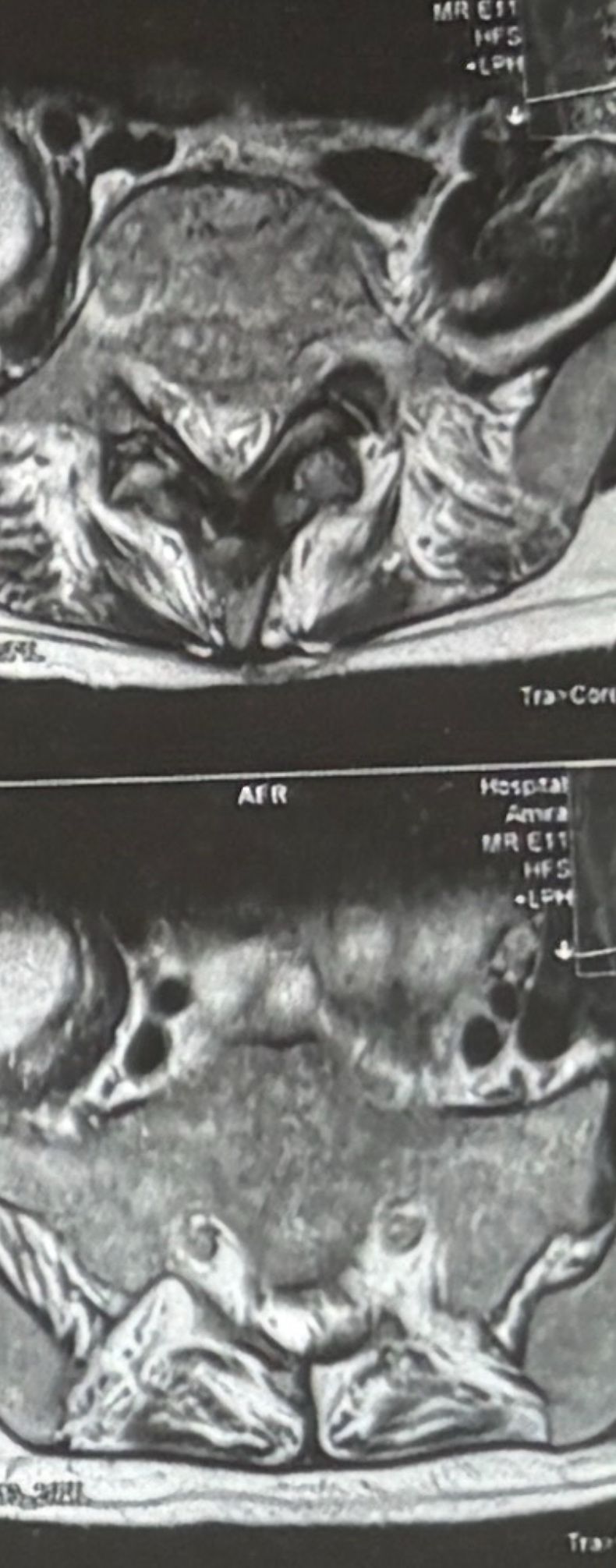
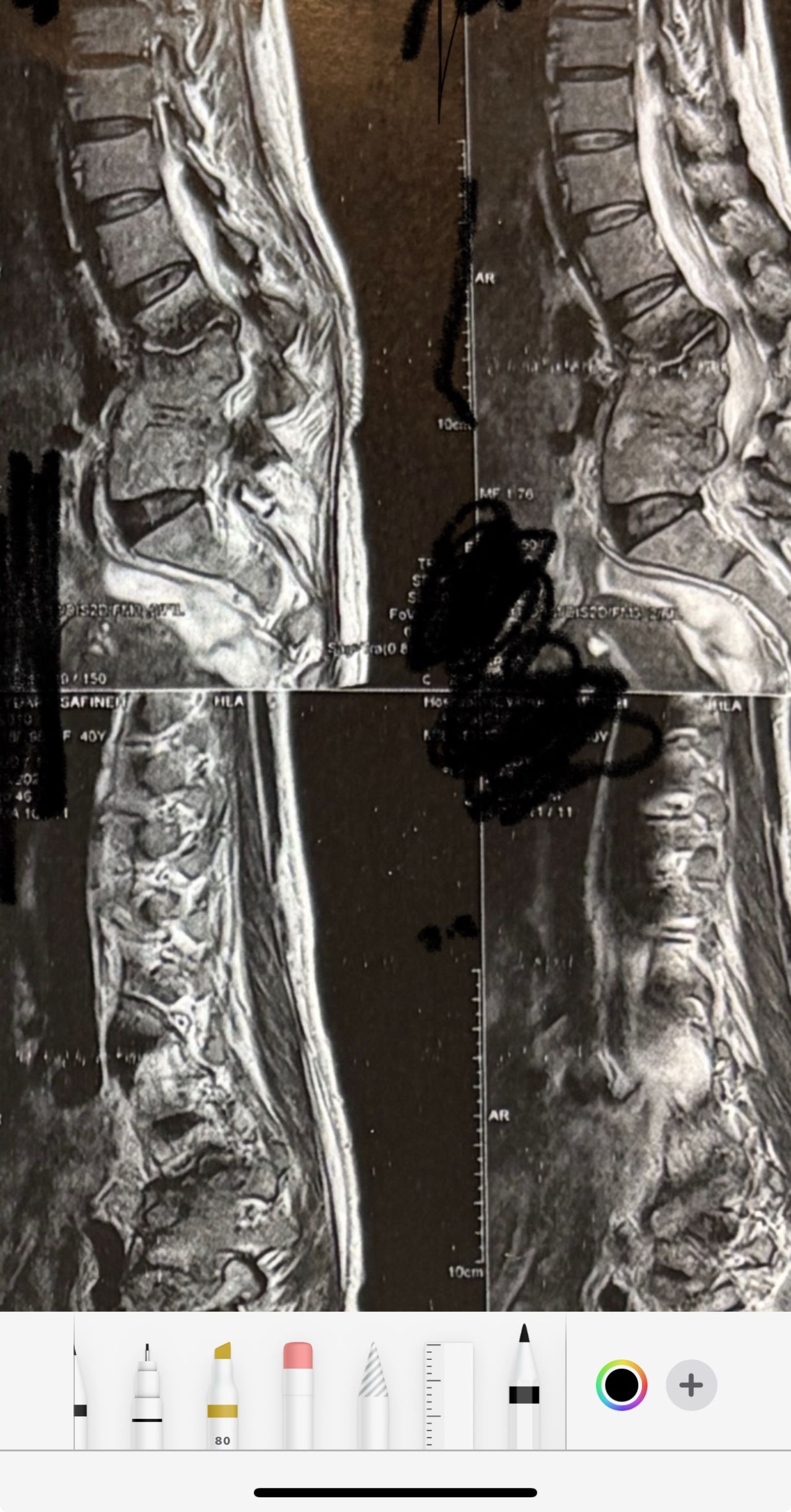
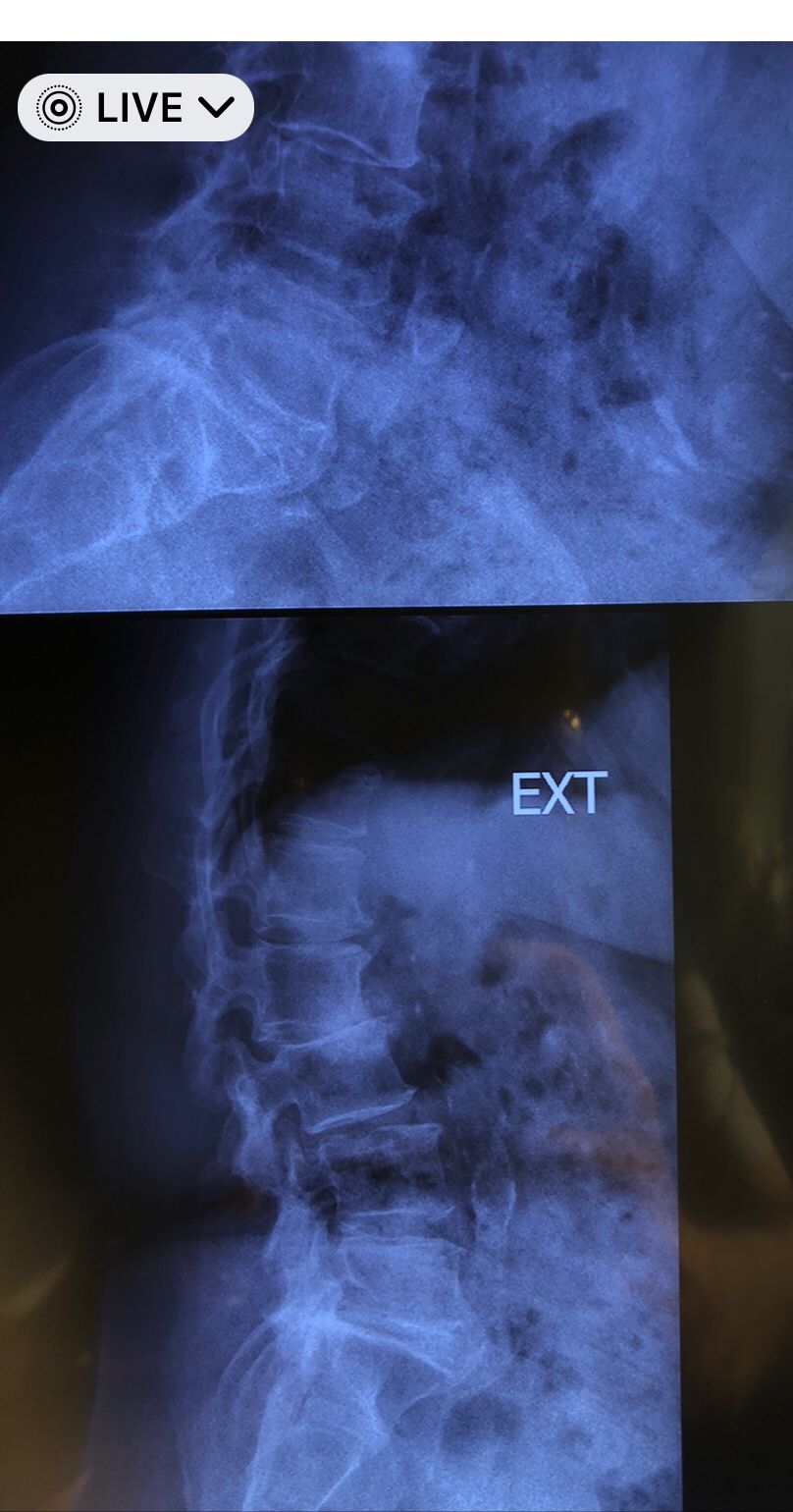
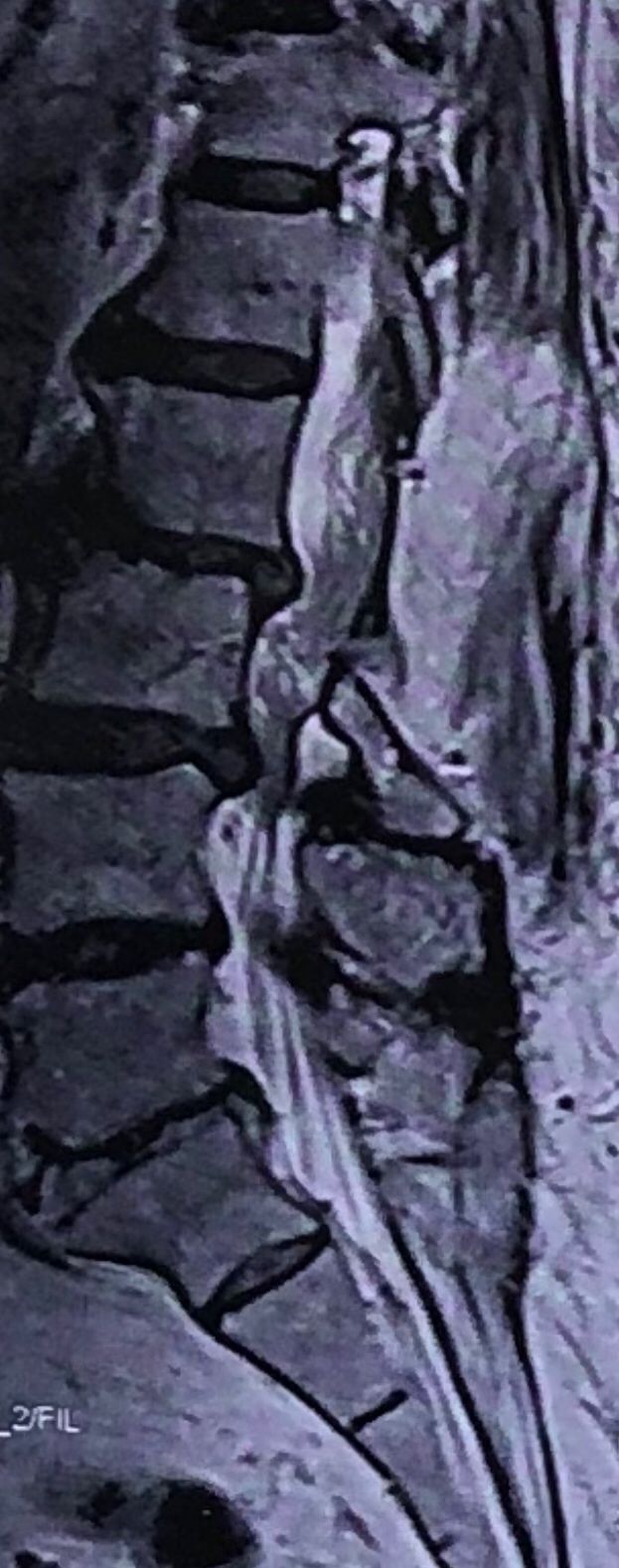
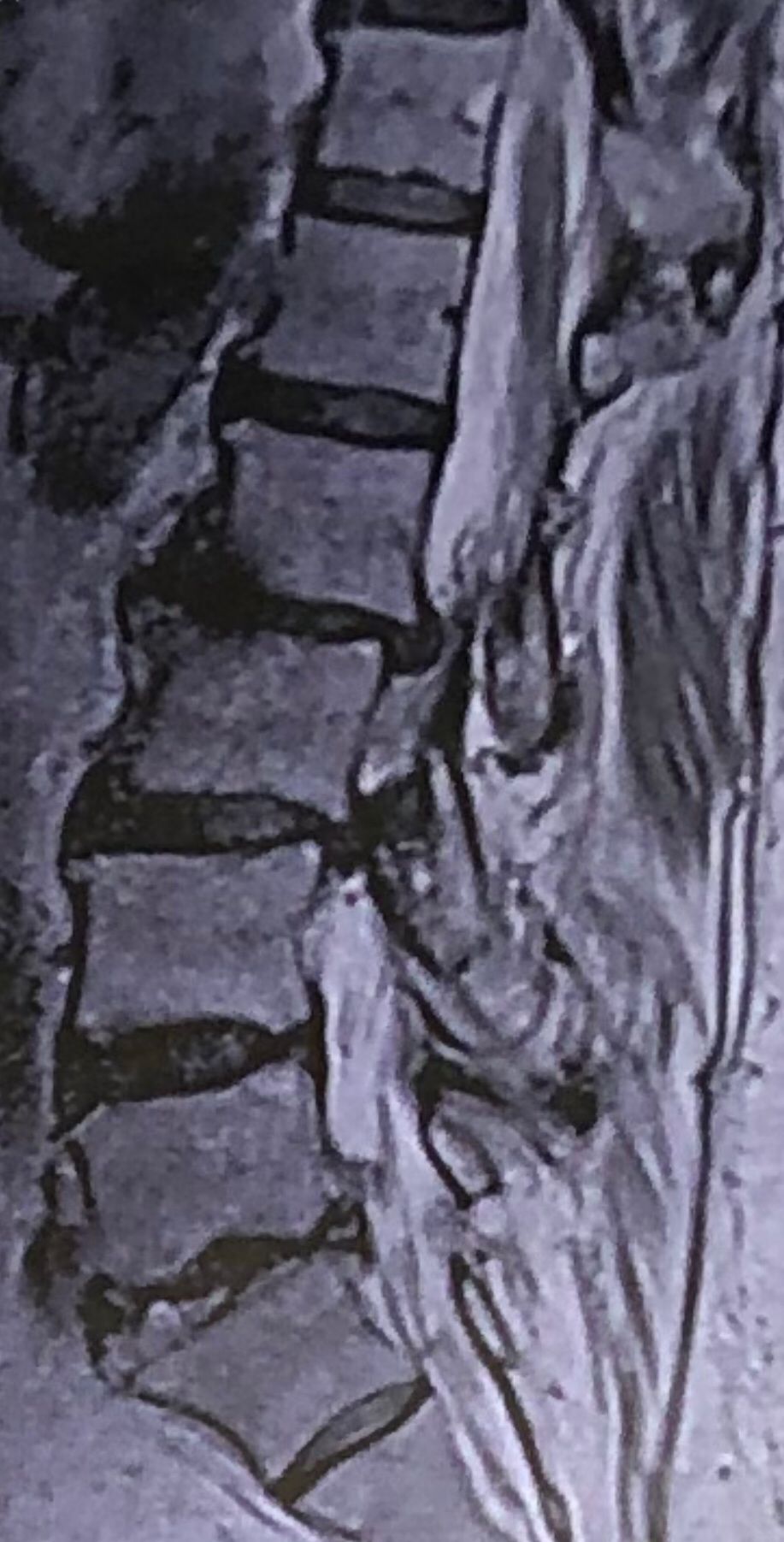
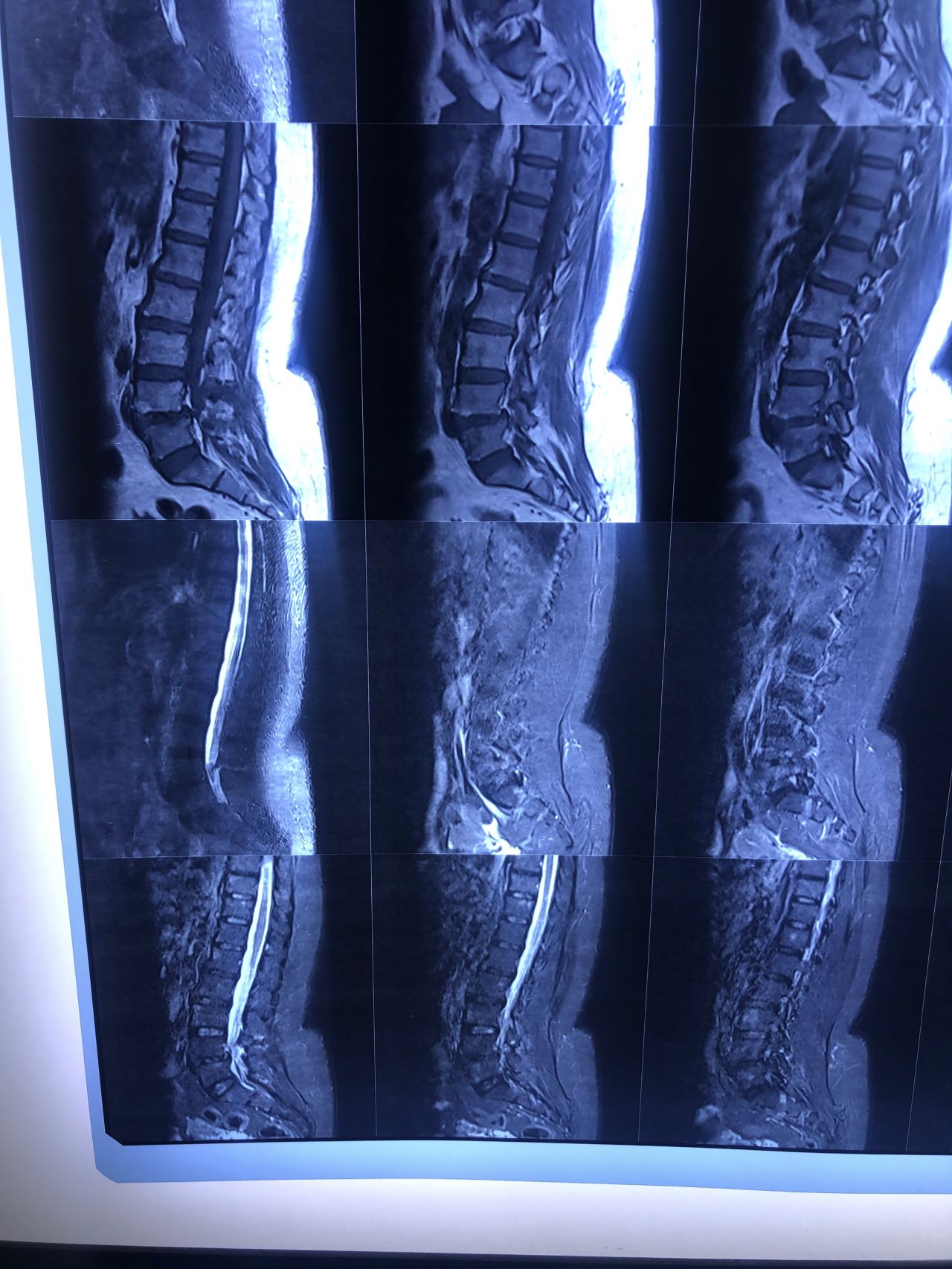
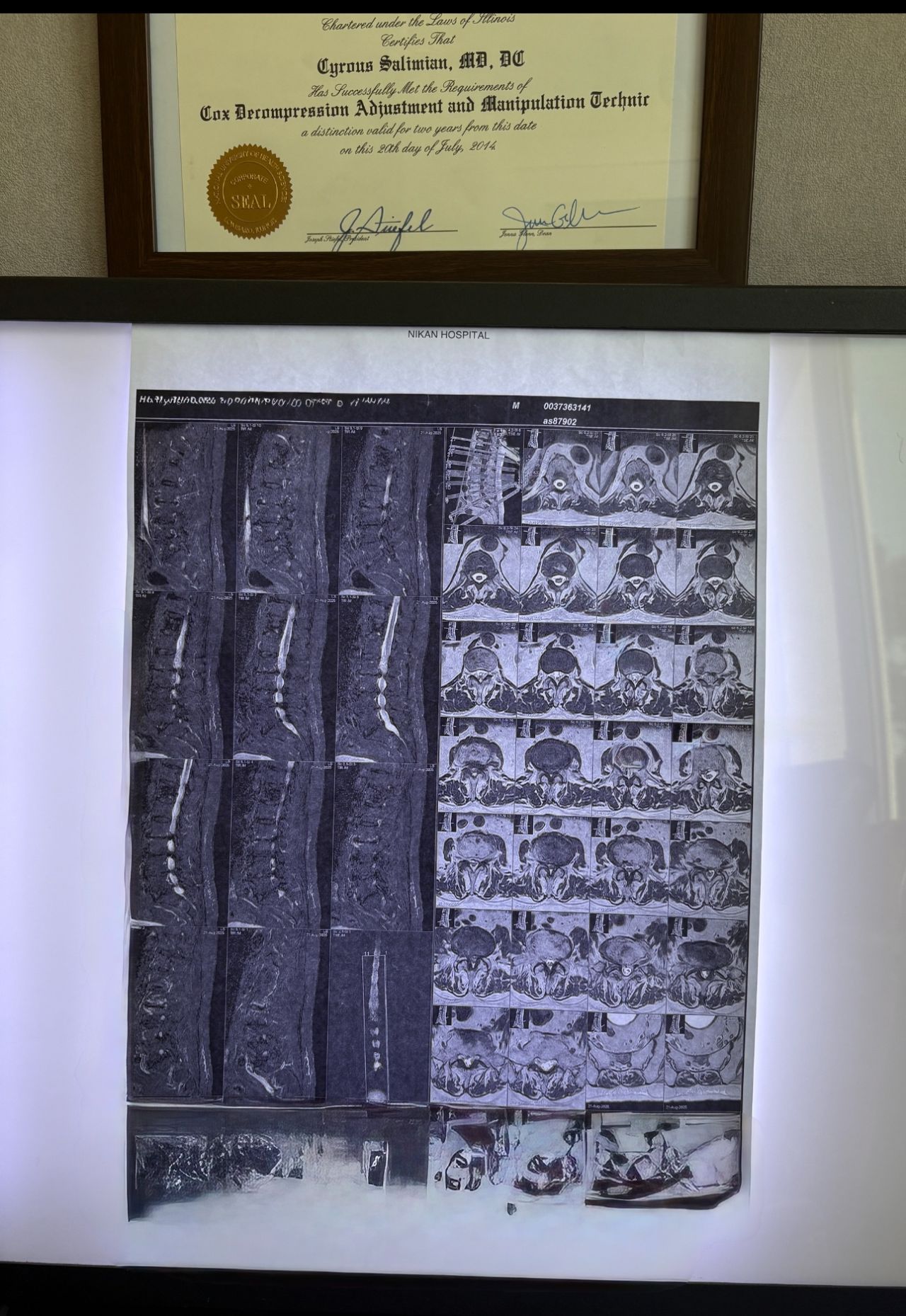
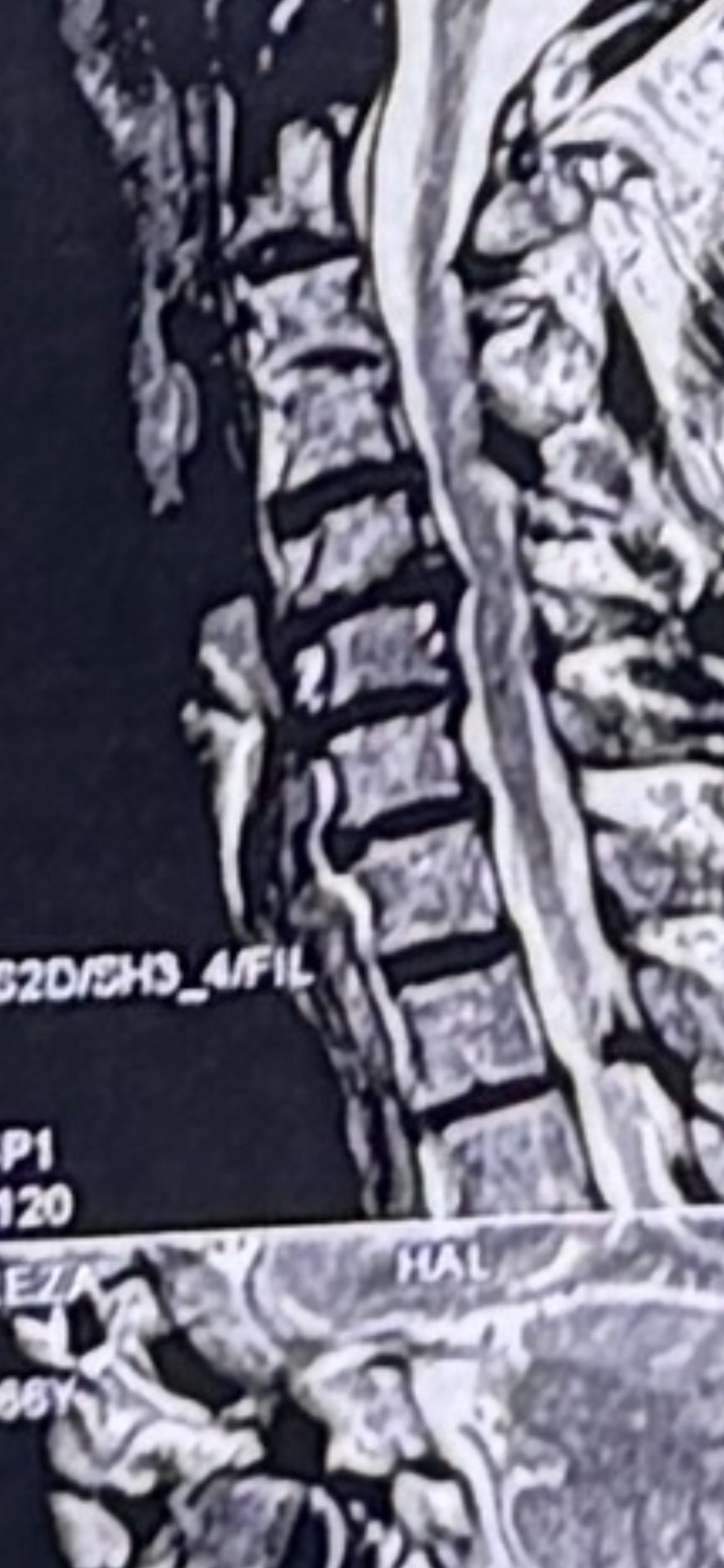
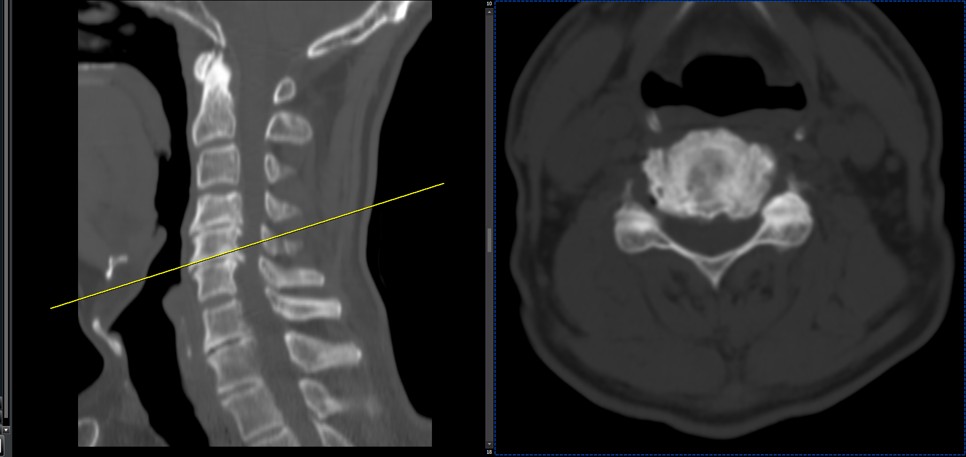
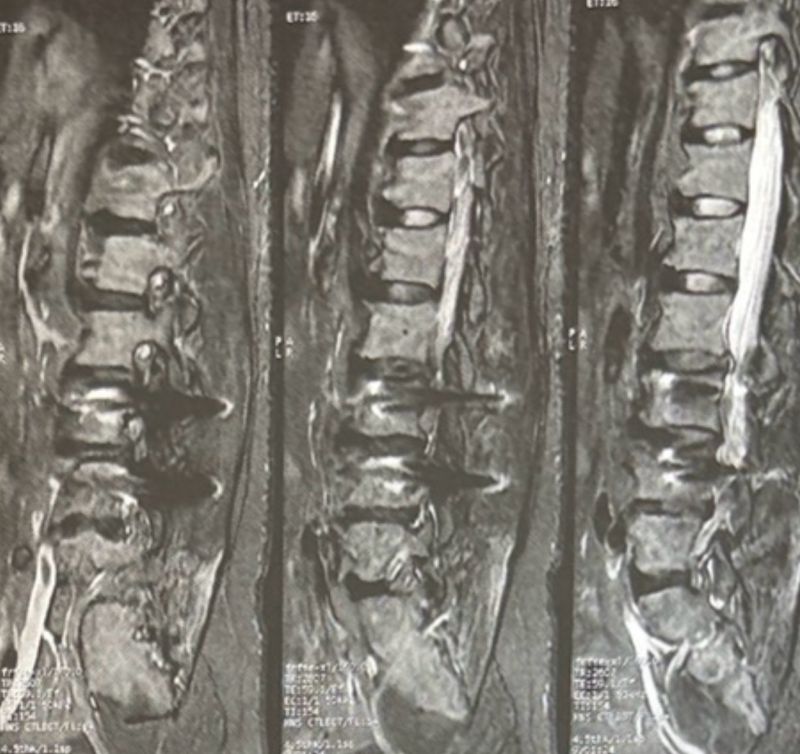
I gave him cervical traction pump to be used 3-5 times per day at home for the next 3 months and i released the patient. He was evaluated every week once for one month and after that every 2 weeks. After 3 month I repeated MRI. Size of the herniated disc was reduced greater than 50 percent. Asked him to do another mri in 6 months


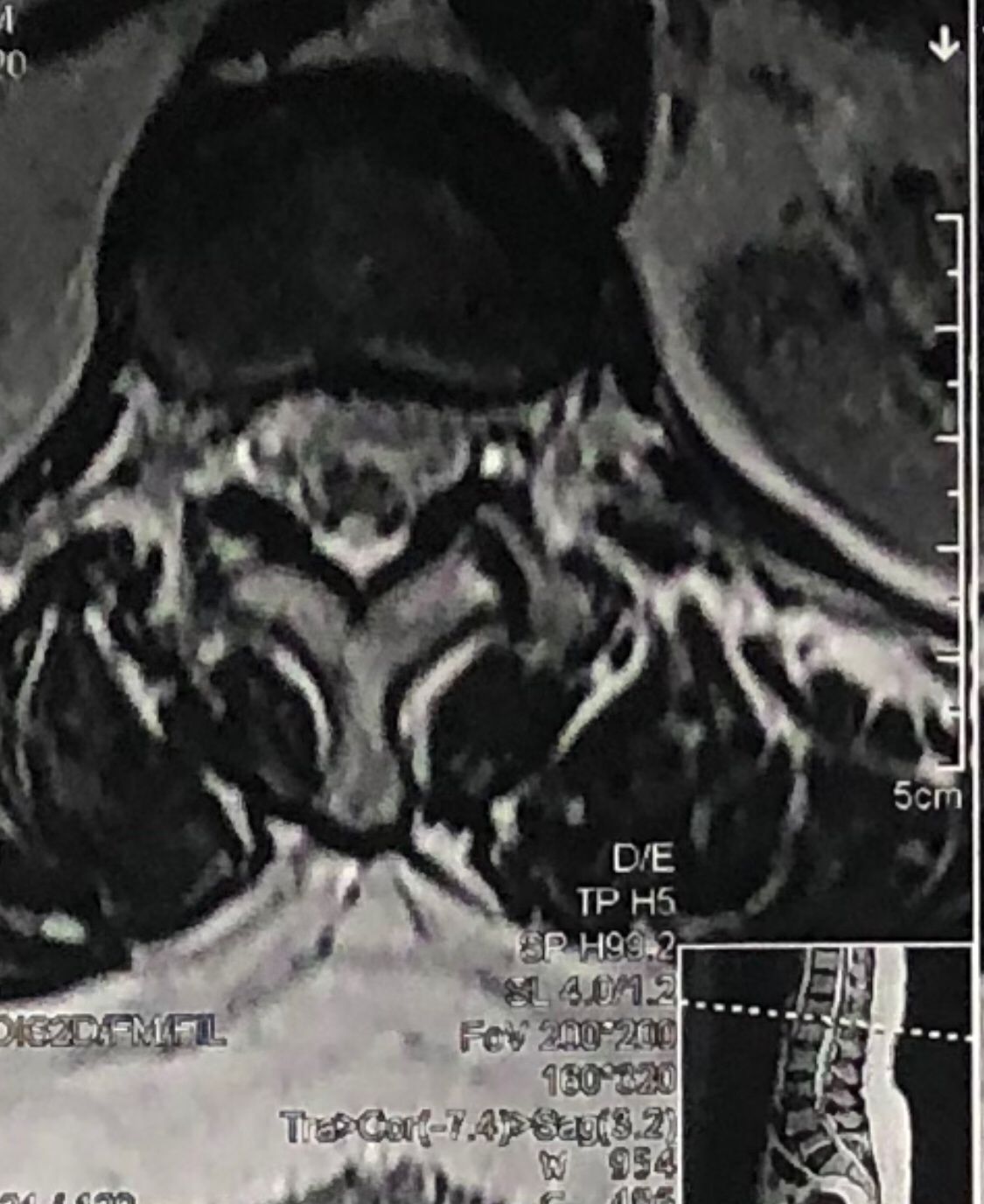
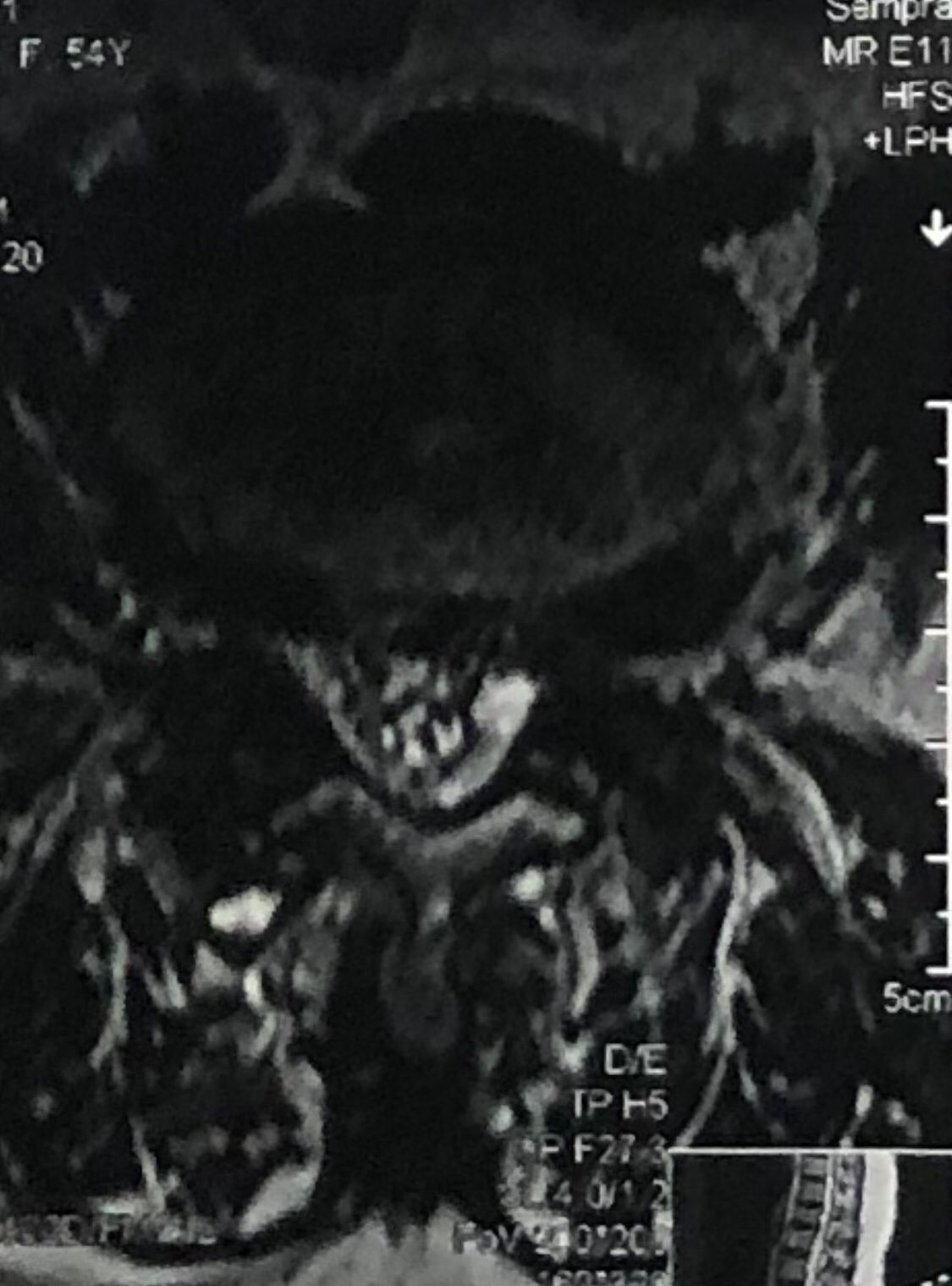
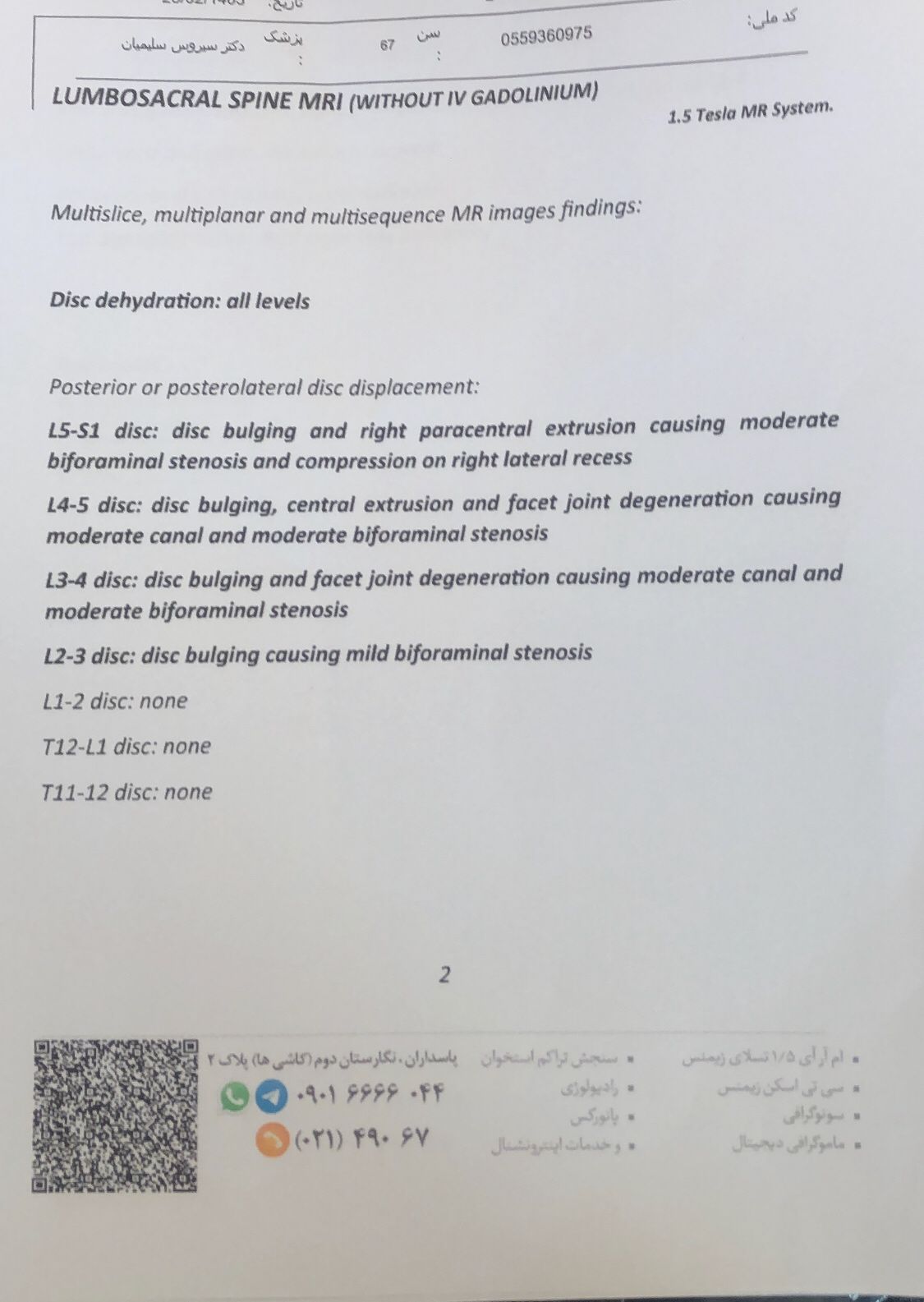
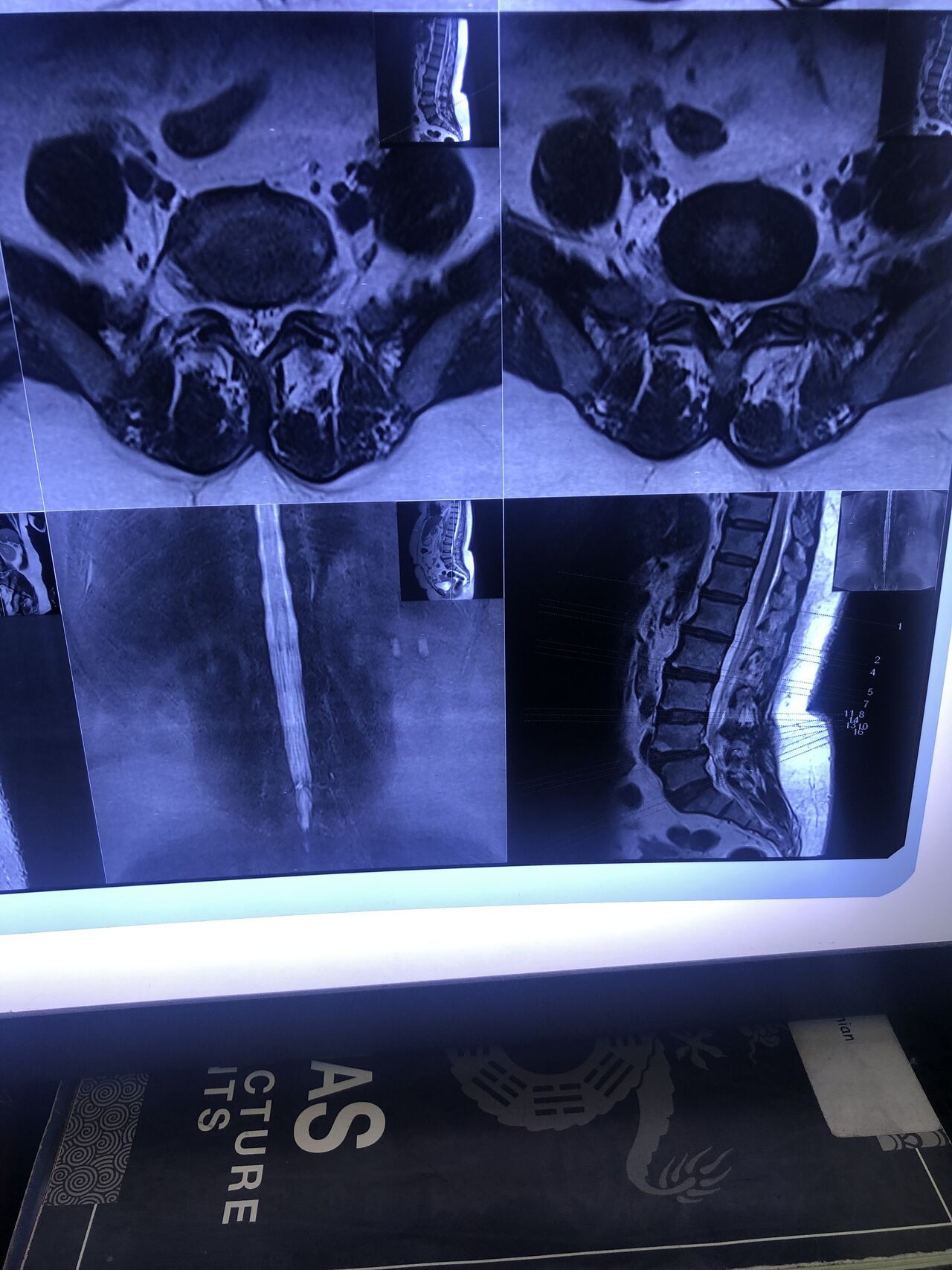
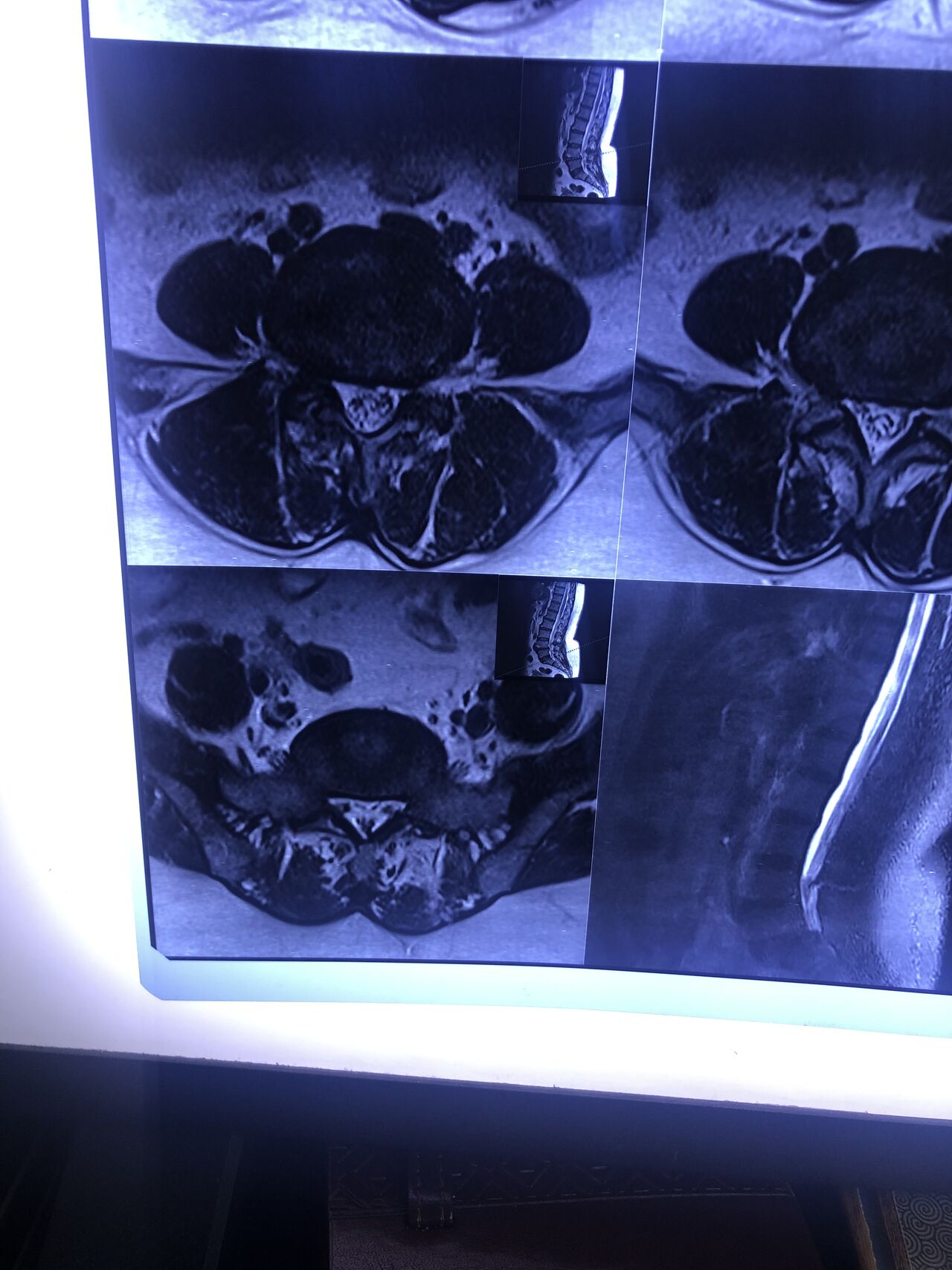
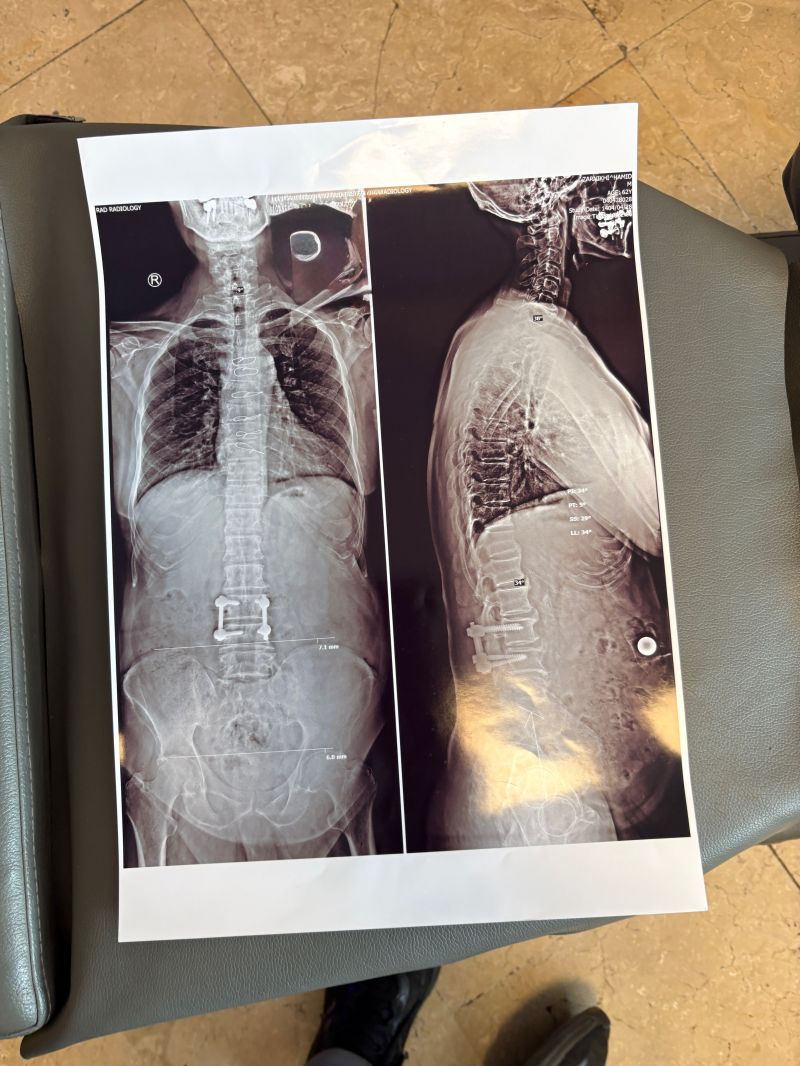
In general: Precise selection of the patients, examination,diagnosis, plan of management, reevaluation and treatment can be done by doctors of chiropractic for the patients with spinal disc herniation and stenosis Moreover giving reasonable time to these kind of patients under direct supervision by their chiropractic doctors can prevent unnecessary surgery. Proper selection of these kind of patients is another important fact that can be done precisely by chiropractors.
MRIs before and after proper management of this patient: